
Child Abuse Imaging — MCQs

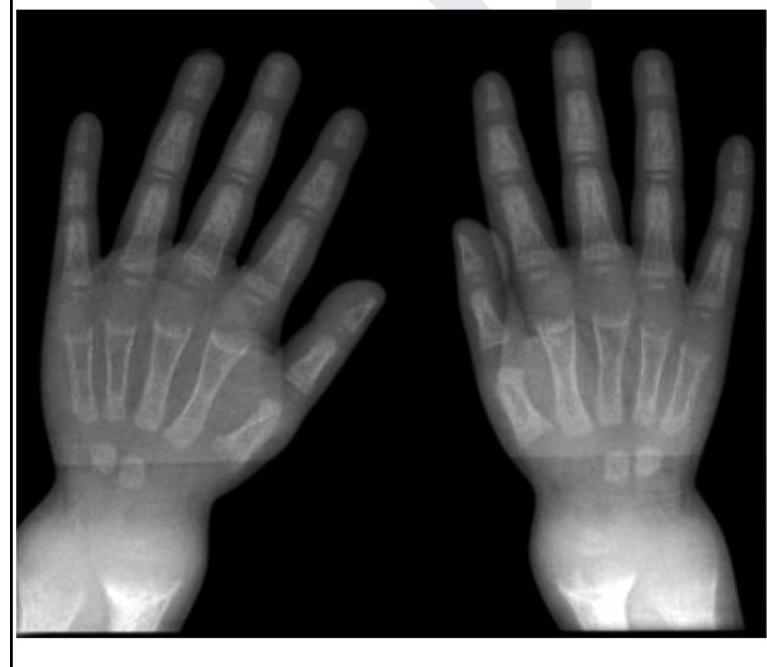
A child presents with poor growth and swelling at joints. A radiograph of his wrist is given below. Lab investigations reveal serum ALP levels of >1500. What is the possible diagnosis?
What is the investigation of choice for diagnosing a stress fracture?
A patient is brought to the emergency following a head-on collision road traffic accident. His BP is 90/60 mmHg. Tachycardia is present. Most likely diagnosis is
A man presents to the emergency department with a head injury following a vehicular accident. What is the investigation of choice?
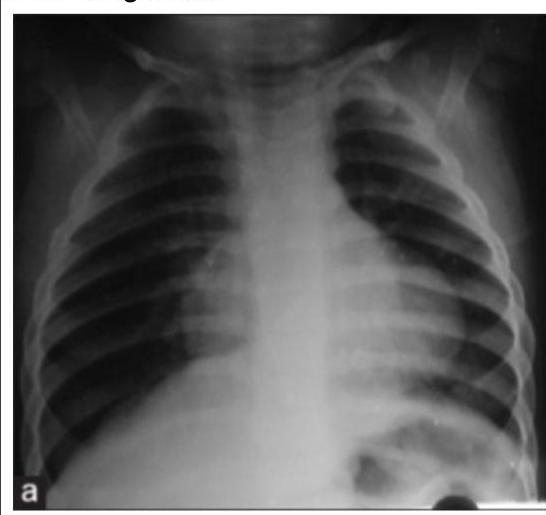
Which of the following is a characteristic feature of Battered Baby Syndrome (Non-Accidental Injury)?
An intrauterine scan at the 13th week of pregnancy showed a fetus with multiple long bone fractures. What is commonly associated with this finding?
A young child presented with mild intermittent upper abdominal pain. X-ray is given below. What is the diagnosis?
Shape of extradural hematoma on NCCT is?
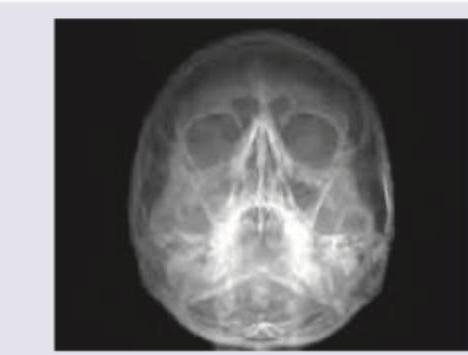
The following X-ray is used to evaluate \qquad sinus?
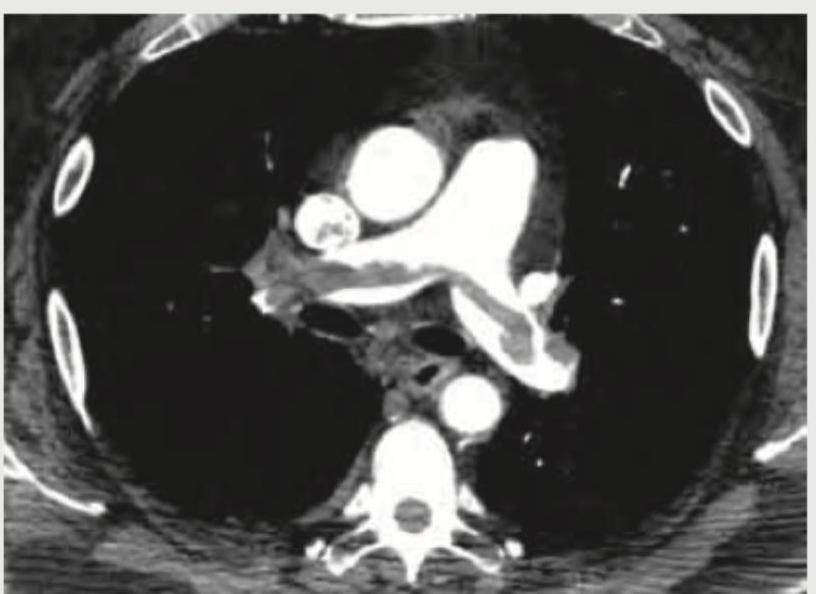
A 35-year-old male with history of 4 weeks of immobilization for fracture of femur develops sudden onset breathlessness and blood in sputum. CT angiography shows? (Recent NEET Pattem 2018-19)
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app