
Pediatric Radiology — MCQs

On this page
The "triangular cord sign" on ultrasonography is indicative of which condition in a neonate?
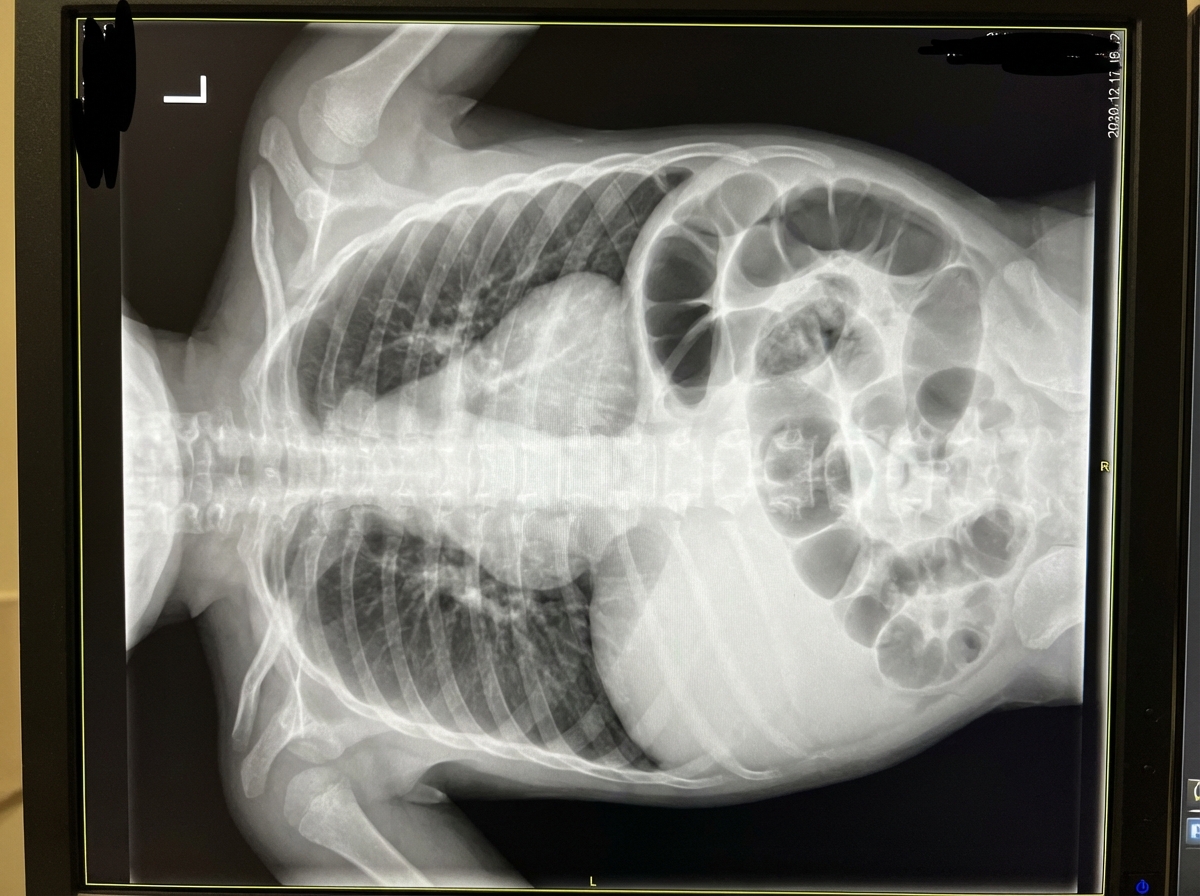
An X-ray of a neonate's abdomen reveals which of the following findings?

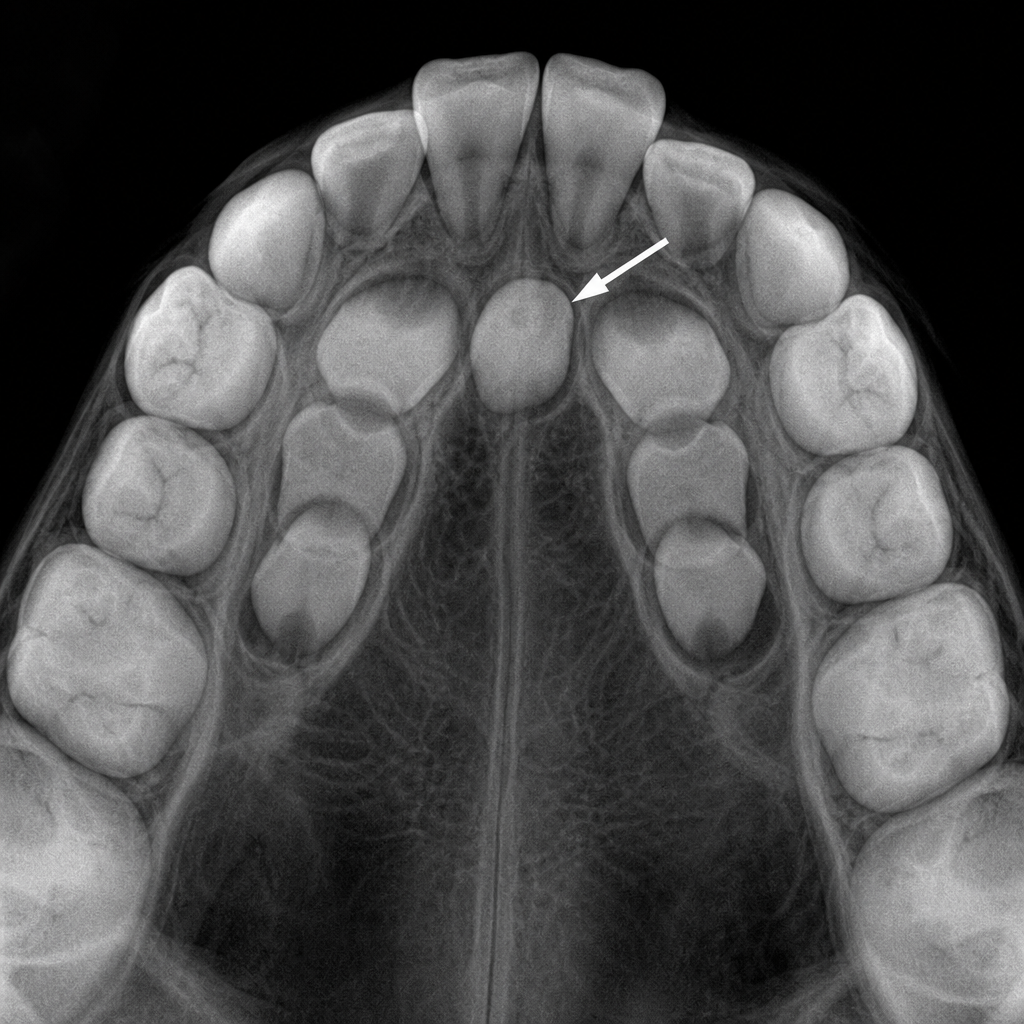
What is the dental anomaly highlighted by the arrow in the occlusal radiograph of an 8-year-old child?
The lung-head ratio is useful in the diagnosis of which of the following conditions?
Given the provided X-ray of a neonate, what is the diagnosis?
Practice by Chapter
Normal Pediatric Developmental Anatomy
Practice Questions
Neonatal Imaging
Practice Questions
Pediatric Chest Imaging
Practice Questions
Pediatric Abdominal Imaging
Practice Questions
Pediatric Musculoskeletal Imaging
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital Heart Disease Imaging
Practice Questions
Pediatric Oncology Imaging
Practice Questions
Child Abuse Imaging
Practice Questions
Pediatric Interventional Radiology
Practice Questions
Radiation Protection in Pediatrics
Practice Questions
Sedation in Pediatric Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app