
Thyroid Scintigraphy — MCQs

Investigation of choice for locating Parathyroid gland:
Which of the following conditions is the most common complication of radioiodine treatment for Graves' disease?
A 26-year-old male presents to the outpatient department with a discrete thyroid swelling. On neck ultrasound, an isolated cystic swelling of the gland is seen. What is the risk of malignancy associated with this finding?
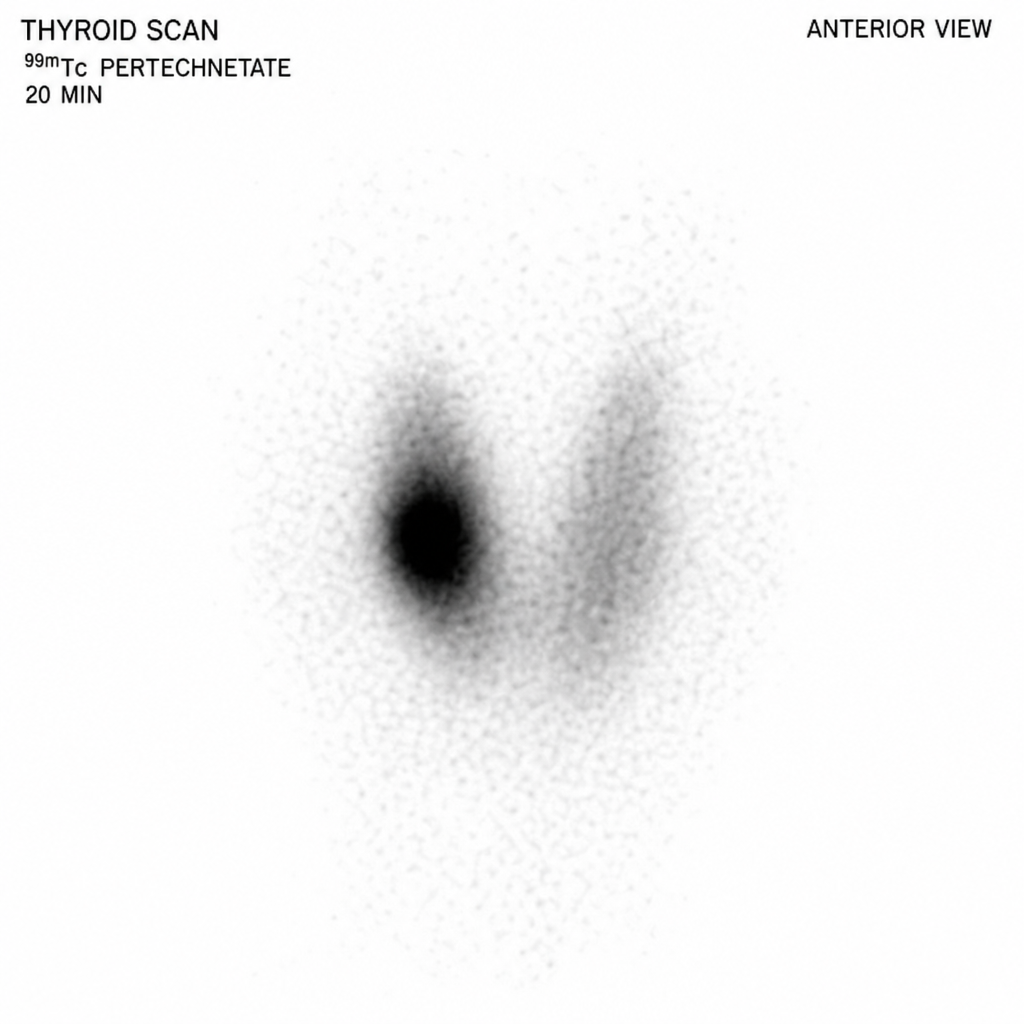
The thyroid scan shown below exhibits a pattern that is most consistent with which of the following disorders?
Most sensitive investigation for preoperative localization of abnormal parathyroid glands is
Which one of the following conditions is diagnosed by Tc99m Pertechnetate Scintigraphy?
A thyroid FNA shows 'bubble gum' colloid. Which nuclear feature would best support papillary thyroid carcinoma?
A 45-year-old female presents with a 2 cm thyroid nodule. Which TIRADS category has >95% risk of malignancy?
Which of the following ultrasound features of a thyroid nodule is not suggestive of malignancy?
What is the best investigation to check for extra thyroid spread of thyroid gland neoplasm ?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app