
Nuclear Medicine — MCQs

On this page
All of the following conditions show increased uptake (hot spot) on a bone scan except?
Which of the following investigations is NOT used in the diagnosis of protein-losing enteropathy?
Which of the following imaging modalities is used to differentiate tumor recurrence from radiation necrosis?
Which is the best scan for assessing myocardial viability?
Which of the following radiopharmaceuticals is used in imaging of the reticuloendothelial system?
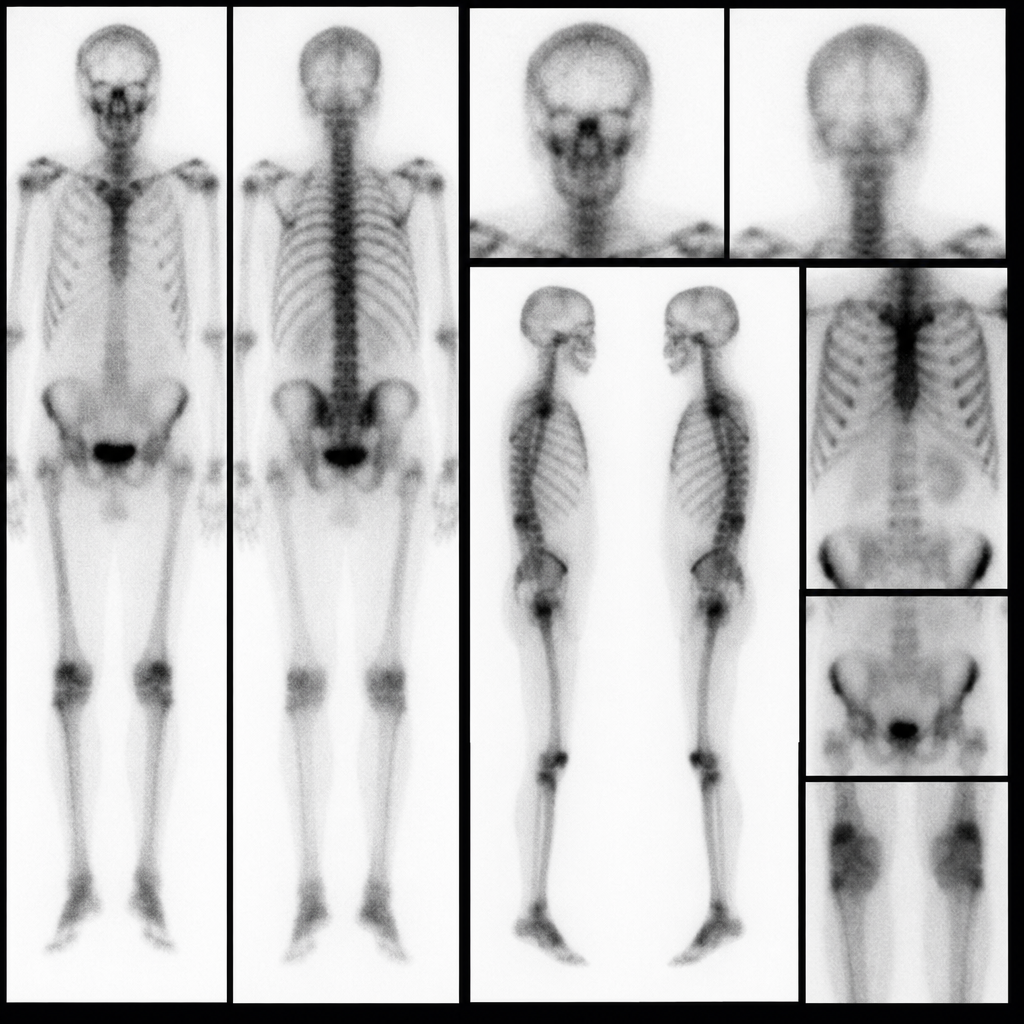
A patient presented with pentad of symptoms: kidney stones, painful bones, abdominal groans, psychic moans, and fatigue. The imaging investigation done for him is shown below. What is this investigation?
Thyroid radioiodine ablation therapy is useful in all except?
Radioactive gold (Au-198) is used in the treatment of which condition?
Which of the following imaging techniques is best able to measure regional brain substrate uptake and metabolic kinetics?
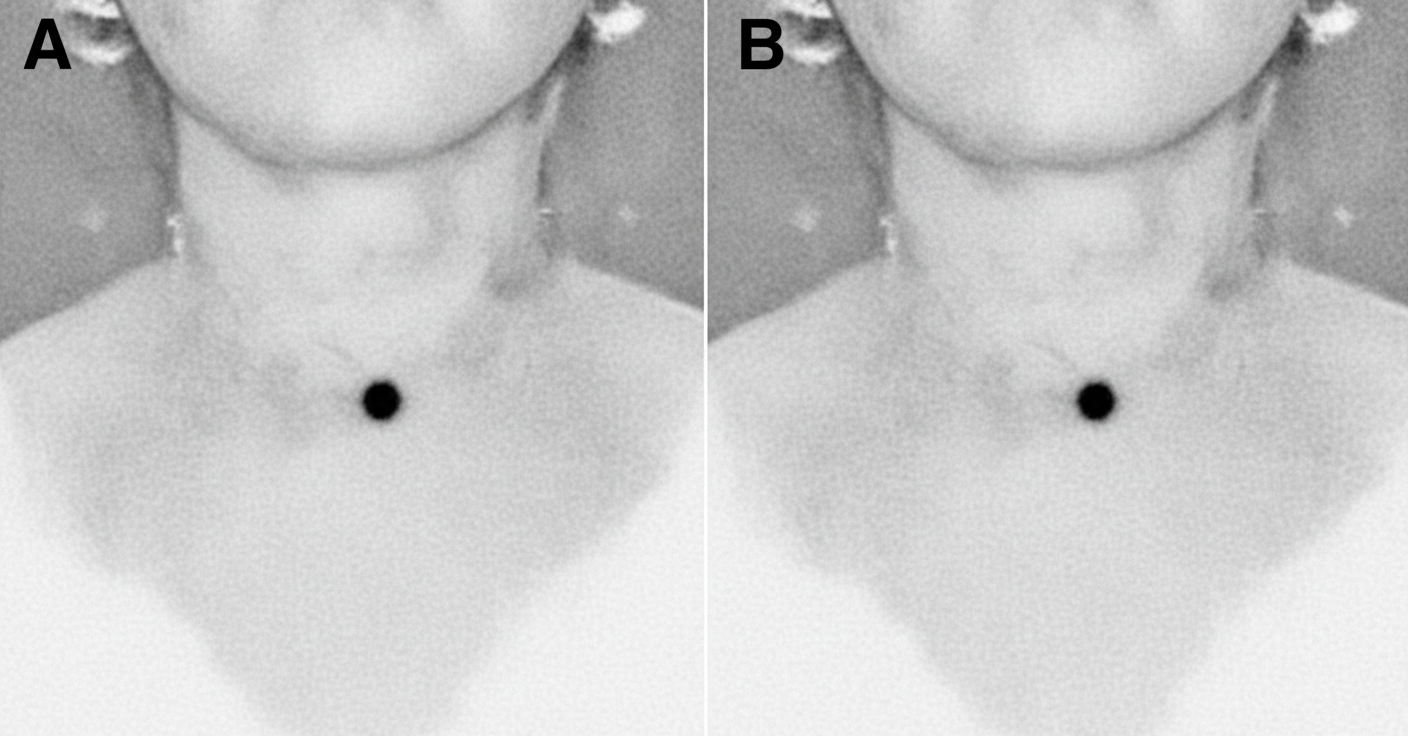
The provided image is a thyroid scan. Based on the scan, what is the most probable diagnosis?
Practice by Chapter
Physics of Nuclear Medicine
Practice Questions
Radiopharmaceuticals
Practice Questions
Radiation Detection in Nuclear Medicine
Practice Questions
Thyroid Scintigraphy
Practice Questions
Bone Scintigraphy
Practice Questions
Renal Nuclear Medicine
Practice Questions
Cardiac Nuclear Medicine
Practice Questions
Pulmonary Nuclear Medicine
Practice Questions
Neurological Nuclear Medicine
Practice Questions
PET/CT Principles and Applications
Practice Questions
Radionuclide Therapy
Practice Questions
Radiation Safety in Nuclear Medicine
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app