
Nuclear Medicine — MCQs

On this page
Half-life of iodine-131 is
Which radionuclide is best suited for measuring glomerular filtration rate (GFR)?
What is the primary function of a gamma camera?
Which of the following is used in the treatment of well-differentiated thyroid carcinoma?
Which investigation is best for assessing the proper functioning of the biliary system?
Which radioisotope is used for treating bone cancer?
Distant bone metastases can be best detected by which of the following imaging techniques?
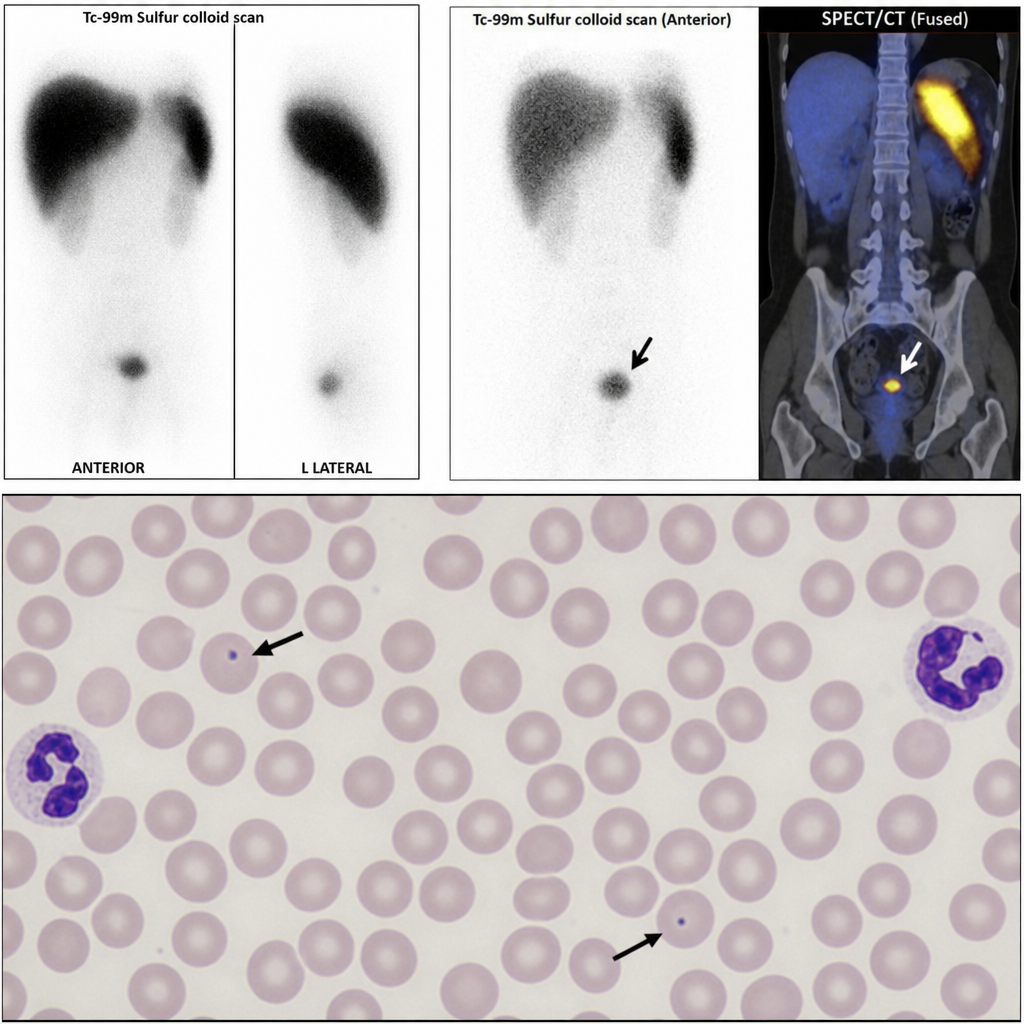
This technetium-99m sulfur colloid scan was performed after the patient presented with abdominal pain. Howell-Jolly bodies were present on a peripheral blood smear. What is the diagnosis?
Isotopes used in the relief of metastatic bone pain include – a) Strontium–89 b) I–131 c) Gold–198 d) P–32 e) Rhenium–186
Which radiopharmaceutical is commonly used in positron emission tomography (PET) imaging?
Practice by Chapter
Physics of Nuclear Medicine
Practice Questions
Radiopharmaceuticals
Practice Questions
Radiation Detection in Nuclear Medicine
Practice Questions
Thyroid Scintigraphy
Practice Questions
Bone Scintigraphy
Practice Questions
Renal Nuclear Medicine
Practice Questions
Cardiac Nuclear Medicine
Practice Questions
Pulmonary Nuclear Medicine
Practice Questions
Neurological Nuclear Medicine
Practice Questions
PET/CT Principles and Applications
Practice Questions
Radionuclide Therapy
Practice Questions
Radiation Safety in Nuclear Medicine
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app