
Nuclear Medicine — MCQs

On this page
In a patient presenting with jaundice, the HIDA scan would be most useful for which of the following:
All the following radioisotopes are used in painful body metastasis except
Radio-isotope of iodine used for thyroid tissue destruction:
Gamma camera in Nuclear Medicine is used for –
MUGA scan is not useful in:
Radioactive isotope of which of the following is used in bone scans?
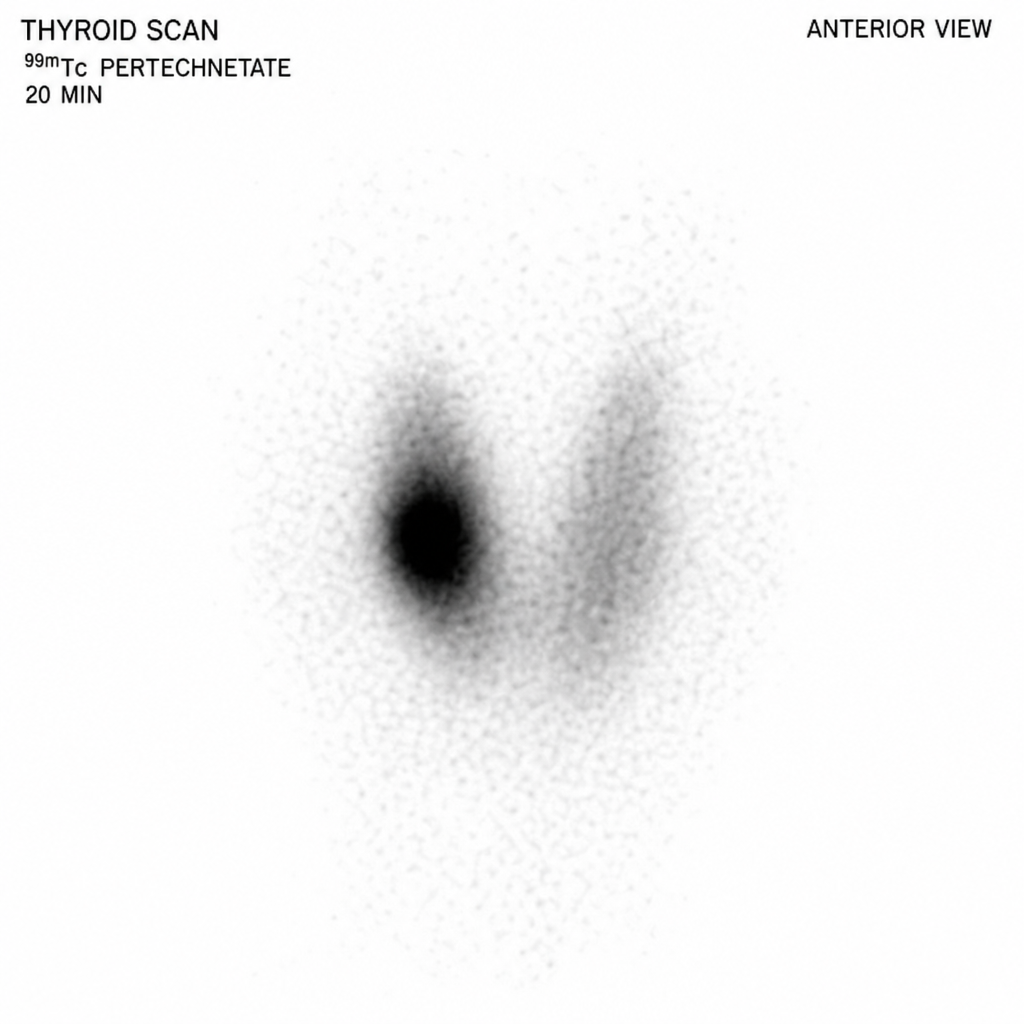
The thyroid scan shown below exhibits a pattern that is most consistent with which of the following disorders?
What is a radionuclide scan finding in hyperparathyroidism?
All of the following radioisotopes are used as systemic radionuclides, EXCEPT:
All isotopes are used for thyroid except:
Practice by Chapter
Physics of Nuclear Medicine
Practice Questions
Radiopharmaceuticals
Practice Questions
Radiation Detection in Nuclear Medicine
Practice Questions
Thyroid Scintigraphy
Practice Questions
Bone Scintigraphy
Practice Questions
Renal Nuclear Medicine
Practice Questions
Cardiac Nuclear Medicine
Practice Questions
Pulmonary Nuclear Medicine
Practice Questions
Neurological Nuclear Medicine
Practice Questions
PET/CT Principles and Applications
Practice Questions
Radionuclide Therapy
Practice Questions
Radiation Safety in Nuclear Medicine
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app