
Nuclear Medicine — MCQs

On this page
The following image shows:

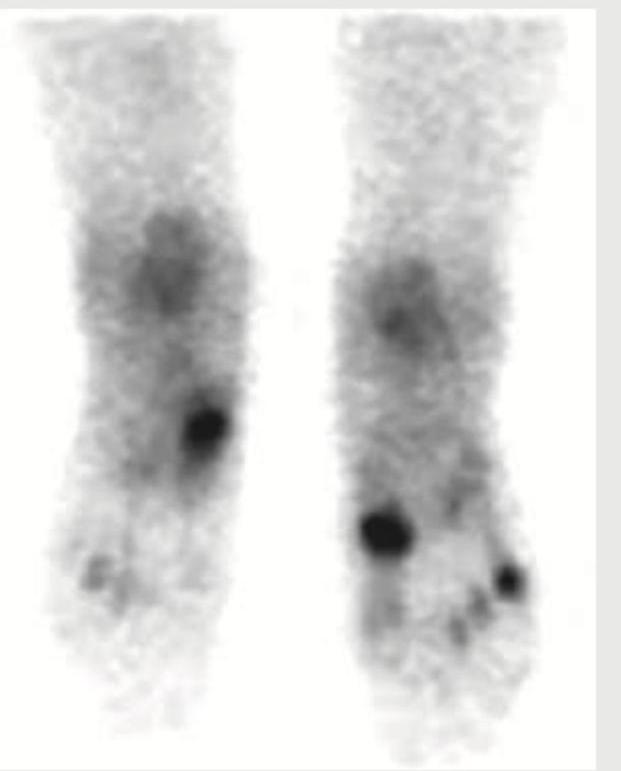
A long distance runner complains of pain in the foot causing reduction in his performance. His X-ray and MRI foot are normal. He was advised to undergo a nuclear scan as shown below. Which tracer is used in this scan? (Recent NEET Pattern 2016-17)
The following image shows: (Recent NEET Pattern 2016-17)

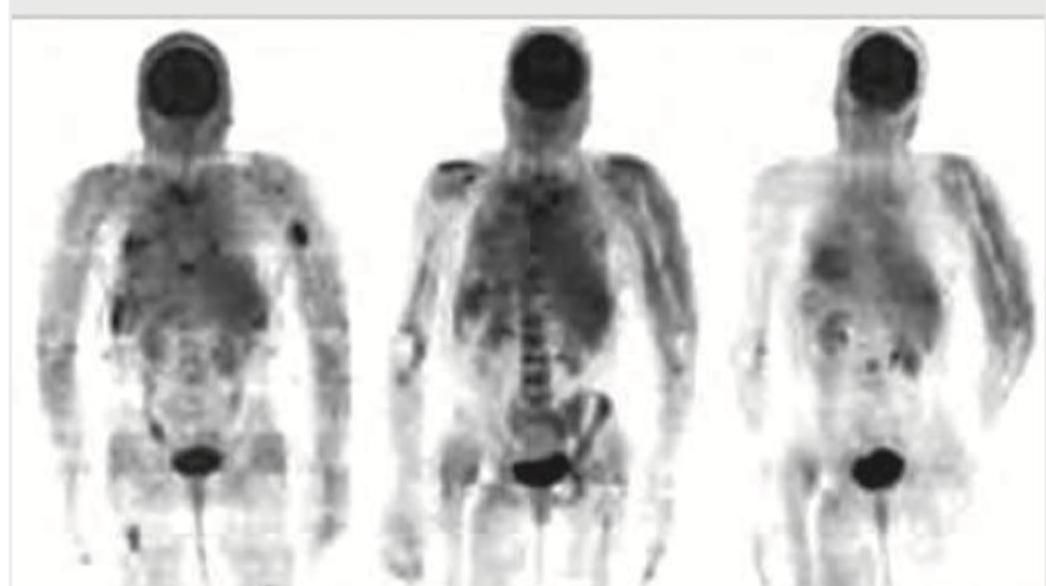
A patient was started on RCHOP regimen for NHL. The investigation shown below was done to monitor response to treatment. What is the investigation?
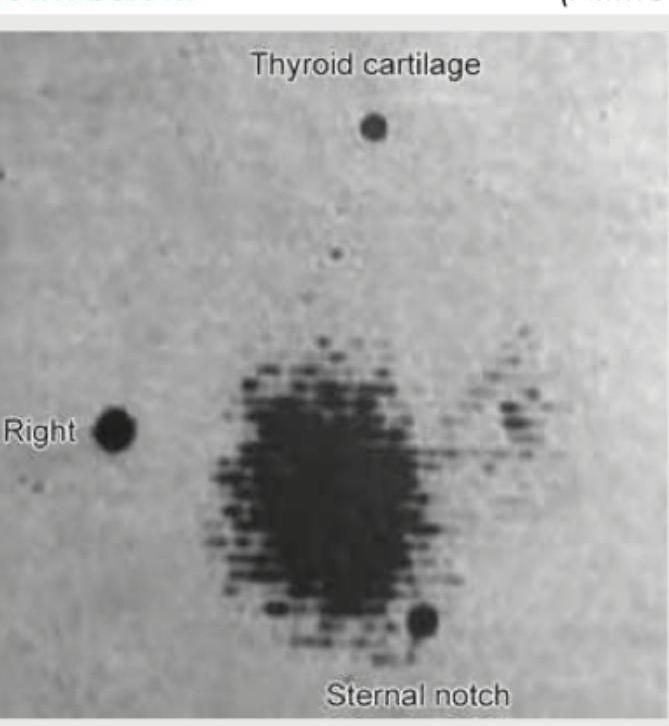
Comment on the diagnosis from the thyroid scan shown below. (AIIMS May 2017)
Positron Emission Tomography (PET) used in Preoperative staging of Gastro Oesophageal tumours is to detect
Best way to localize extra-adrenal pheochromocytoma:
Radiopharmaceutical used for phagocyte study scan:
Hot spot in heart is seen in which scan
Which radioisotope is PRIMARILY used for detecting acute myocardial infarction rather than assessing myocardial perfusion?
Practice by Chapter
Physics of Nuclear Medicine
Practice Questions
Radiopharmaceuticals
Practice Questions
Radiation Detection in Nuclear Medicine
Practice Questions
Thyroid Scintigraphy
Practice Questions
Bone Scintigraphy
Practice Questions
Renal Nuclear Medicine
Practice Questions
Cardiac Nuclear Medicine
Practice Questions
Pulmonary Nuclear Medicine
Practice Questions
Neurological Nuclear Medicine
Practice Questions
PET/CT Principles and Applications
Practice Questions
Radionuclide Therapy
Practice Questions
Radiation Safety in Nuclear Medicine
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app