
Nuclear Medicine — MCQs

On this page
Which of the following imaging modalities is used to assess the distribution of functional renal tissue?
Radioisotope used in PET-CT scan?
Ga-68 PSMA PET scan is used to diagnose which of the following conditions?
A patient presented to OPD with complaints of fatigue, loss of appetite, constipation, urinary symptoms of kidney stone, and increased urination. The patient has a history of psychiatric disorder; you suspect a case of hyperparathyroidism. Which of the following investigations is useful in this condition?
A 30-year-old woman presented with complaints of bone pain and abdominal cramps. Her family says she has a history of abnormal behavior. The consultant doctor arrived at a provisional diagnosis based on the clinical features. Which of the following would be the best investigation to arrive at a definitive diagnosis?
Which of the following is the best imaging modality to diagnose neuroendocrine tumors (NETs)?
A patient who was diagnosed with prostate cancer is being investigated. The bone scan is reported as a super scan with increased uptake in the bones and reduced activity in the spleen. What is the reason for this super scan appearance?
What is the most useful investigation for localization of a parathyroid adenoma?
The scintigraphic image shows heterogeneous uptake with multiple hot and cold areas. Identify the organ depicted.
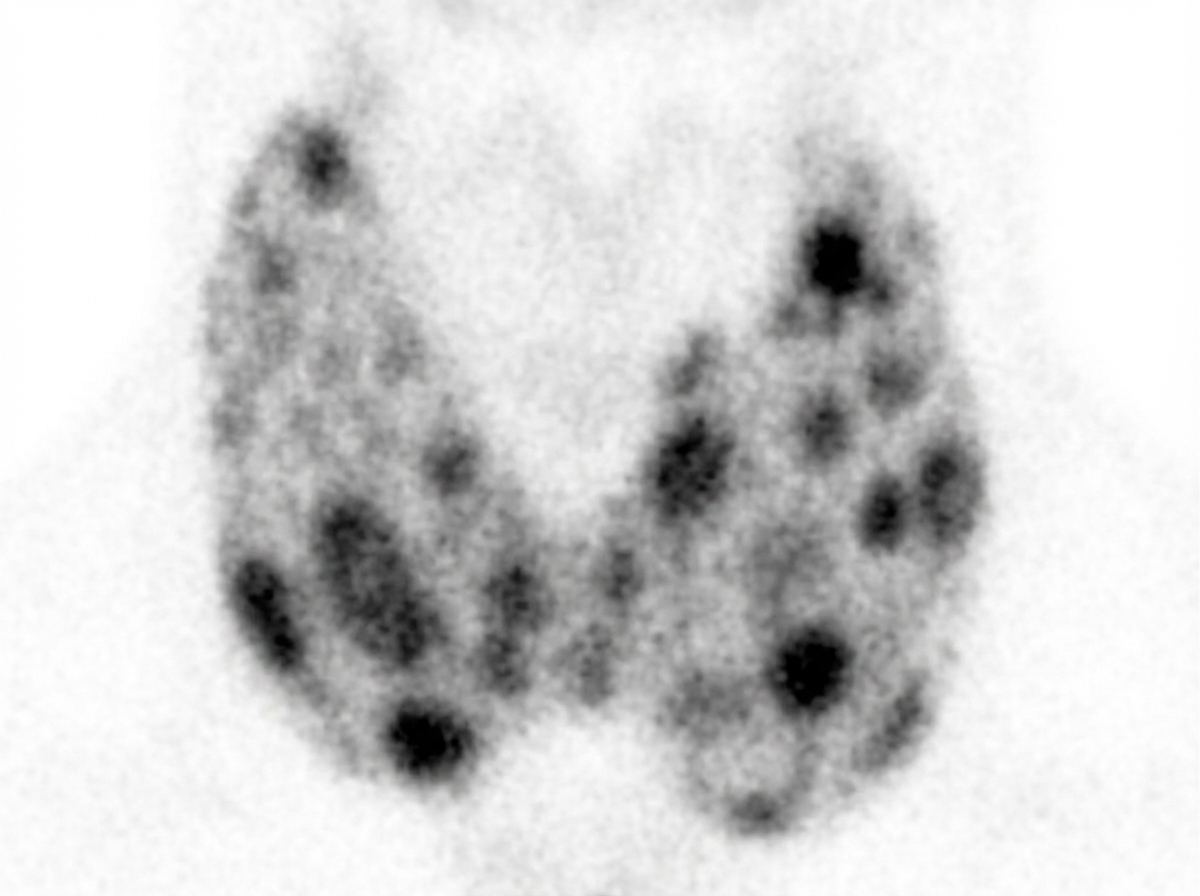
All of the following agents are used in the imaging technique shown below except:

Practice by Chapter
Physics of Nuclear Medicine
Practice Questions
Radiopharmaceuticals
Practice Questions
Radiation Detection in Nuclear Medicine
Practice Questions
Thyroid Scintigraphy
Practice Questions
Bone Scintigraphy
Practice Questions
Renal Nuclear Medicine
Practice Questions
Cardiac Nuclear Medicine
Practice Questions
Pulmonary Nuclear Medicine
Practice Questions
Neurological Nuclear Medicine
Practice Questions
PET/CT Principles and Applications
Practice Questions
Radionuclide Therapy
Practice Questions
Radiation Safety in Nuclear Medicine
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app