
Nuclear Medicine — MCQs

On this page
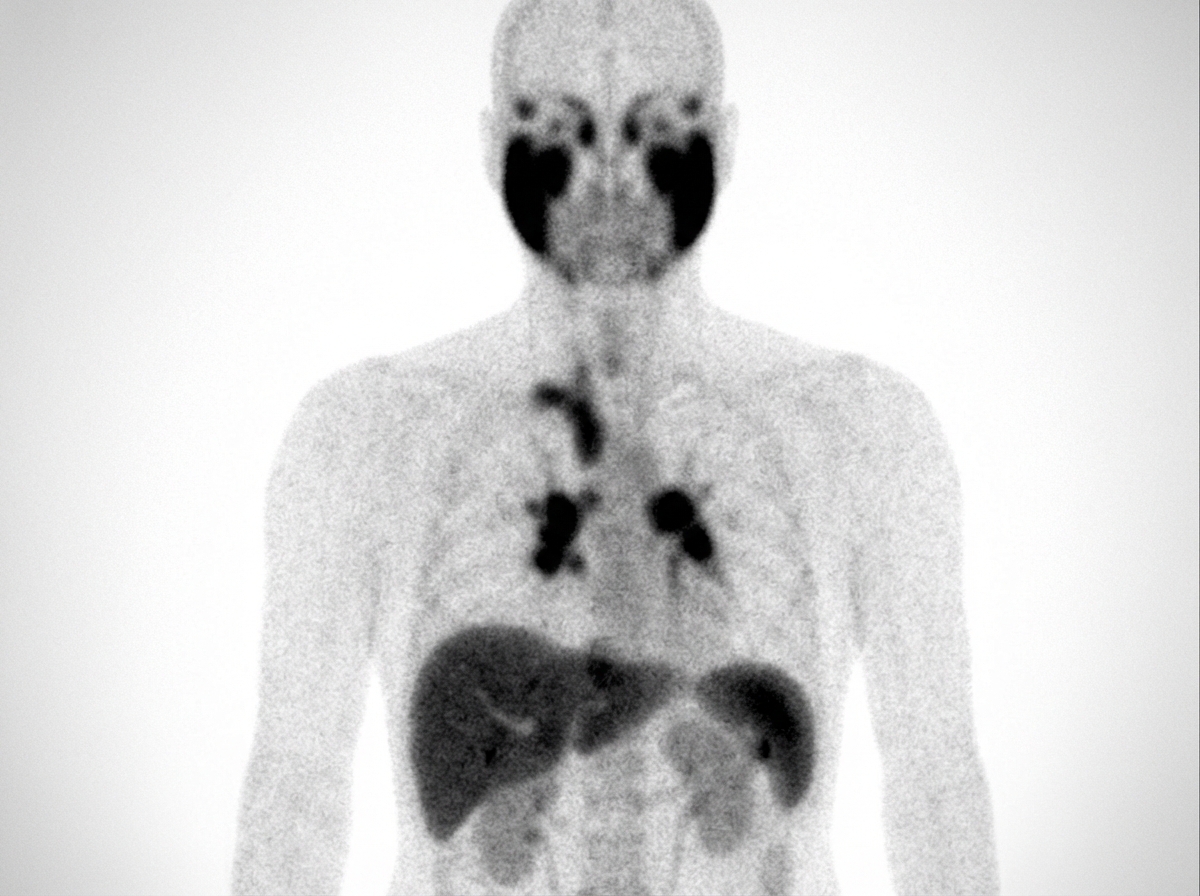
What diagnosis is implied by the results of this gallium scan?
Which of the following statements about isotope scanning of the thyroid is FALSE?
Which one of the following conditions is diagnosed by Tc-99m Pertechnetate Scintigraphy?
What is the modality of choice for screening of bony metastases?
What is the gold standard method for detecting renal scarring in a patient with recurrent urinary tract infection?
Whole-body iodine scan after total thyroidectomy is not recommended for which type of thyroid cancer?
What is the investigation of choice for detecting renal scarring defects?
What is true about PET scan?
All are true about 18 FDG PET scanning except?
Which bone scan is used to detect bone metastasis?
Practice by Chapter
Physics of Nuclear Medicine
Practice Questions
Radiopharmaceuticals
Practice Questions
Radiation Detection in Nuclear Medicine
Practice Questions
Thyroid Scintigraphy
Practice Questions
Bone Scintigraphy
Practice Questions
Renal Nuclear Medicine
Practice Questions
Cardiac Nuclear Medicine
Practice Questions
Pulmonary Nuclear Medicine
Practice Questions
Neurological Nuclear Medicine
Practice Questions
PET/CT Principles and Applications
Practice Questions
Radionuclide Therapy
Practice Questions
Radiation Safety in Nuclear Medicine
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app