
Cardiac Nuclear Medicine — MCQs

Cardiotoxicity caused by radiotherapy & chemotherapy is best detected by
MUGA scan is not useful in:
Hot spot in heart is seen in which scan
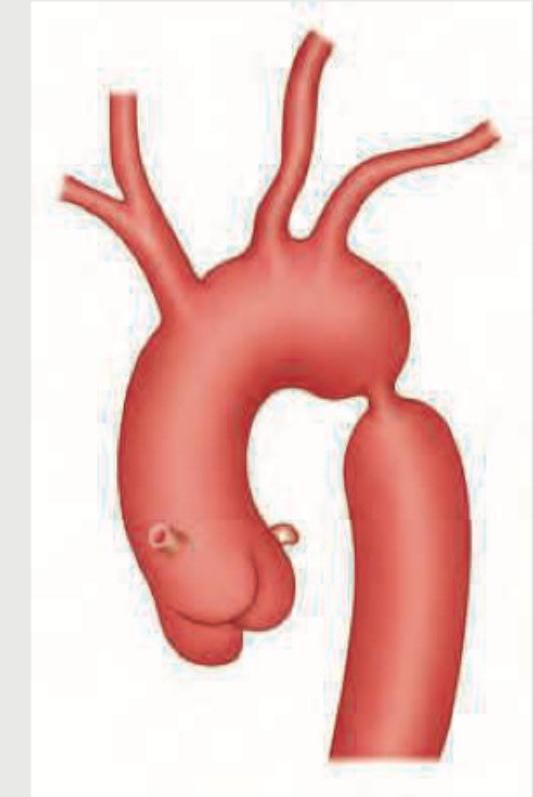
In the condition shown below, rib notching is present in which of the following ribs? (AIIMS Nov 2015)
What is the best investigation to check for extra thyroid spread of thyroid gland neoplasm ?
In designing a clinical protocol for PSMA PET imaging in prostate cancer, which combination of factors would provide optimal image quality while minimizing radiation exposure?
A patient with treated breast cancer shows a liver lesion on CT. FDG-PET shows SUVmax of 2.8 in the lesion. Follow-up scan after 3 months shows increase in size but SUVmax decreased to 1.9. What is the most likely explanation?
A 45-year-old diabetic patient presents for FDG-PET scan for lymphoma staging. Blood glucose is 220 mg/dL. What is the most appropriate management before proceeding with imaging?
What is the underlying principle behind FDG uptake in malignant cells during PET imaging?
What is the physical half-life of Fluorine-18 used in PET imaging?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app