
Spine Imaging: Trauma and Degenerative Disease — MCQs

What is the investigation of choice for diagnosing a stress fracture?
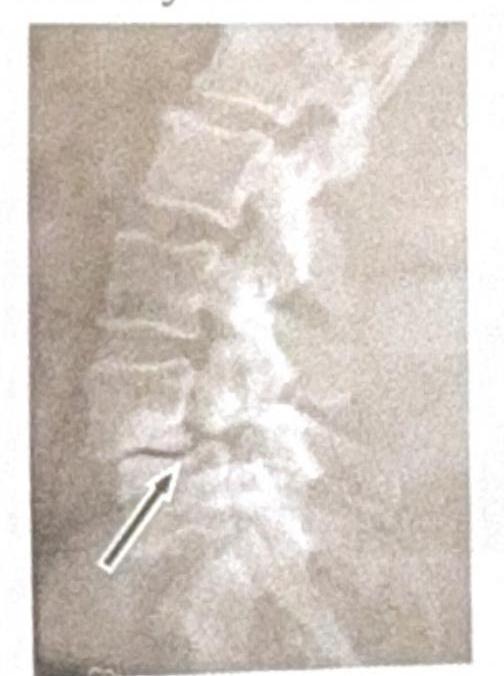
A 75-year-old female has chronic backache. X-ray of the spine is shown. What is the most likely diagnosis?

What is the investigation of choice in a patient with traumatic paraplegia?
A lady had a trauma to the neck. X-ray is attached. What is the diagnosis?

Identify the condition shown in the image:
After chronic use of steroids severe pain in right hip with immobility is due to
Spine MRI shows 'pencil-sharpened' vertebral bodies and 'H-shaped' vertebrae on T1-weighted images. Most likely diagnosis?
A patient with a history of chronic ear infection now presents with manifestations, including headache and vomiting. A CT brain image is shown. What is the most probable diagnosis?

Time of Flight technique is employed in —
What is the primary imaging modality used for diagnosing urethral trauma?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app