
Neuroradiology — MCQs

On this page
A dumbbell tumor is a characteristic feature of which of the following neoplasms?
What is the characteristic MRI brain appearance described as a 'soap bubble'?
Which of the following tend to show marked and homogeneous enhancement on Gd-DTPA enhanced MRI?
A patient was diagnosed with intracranial cavernous angioma on MR scan. What MRI finding is characteristic of this lesion?
What is the stage of neurocysticercosis characterized by a visible cyst with a scolex and minimal edema?
A 40-year-old female patient presented with recurrent headaches. MRI showed an extra-axial, dural-based, and enhancing lesion. What is the most likely diagnosis?
Which of the following lesions characteristically shows a biconvex shape on CT scan?
Bilateral symmetrical basal ganglia calcification is seen with which condition?
On MR-spectroscopy, what peak is typically seen at 3.2 ppm?
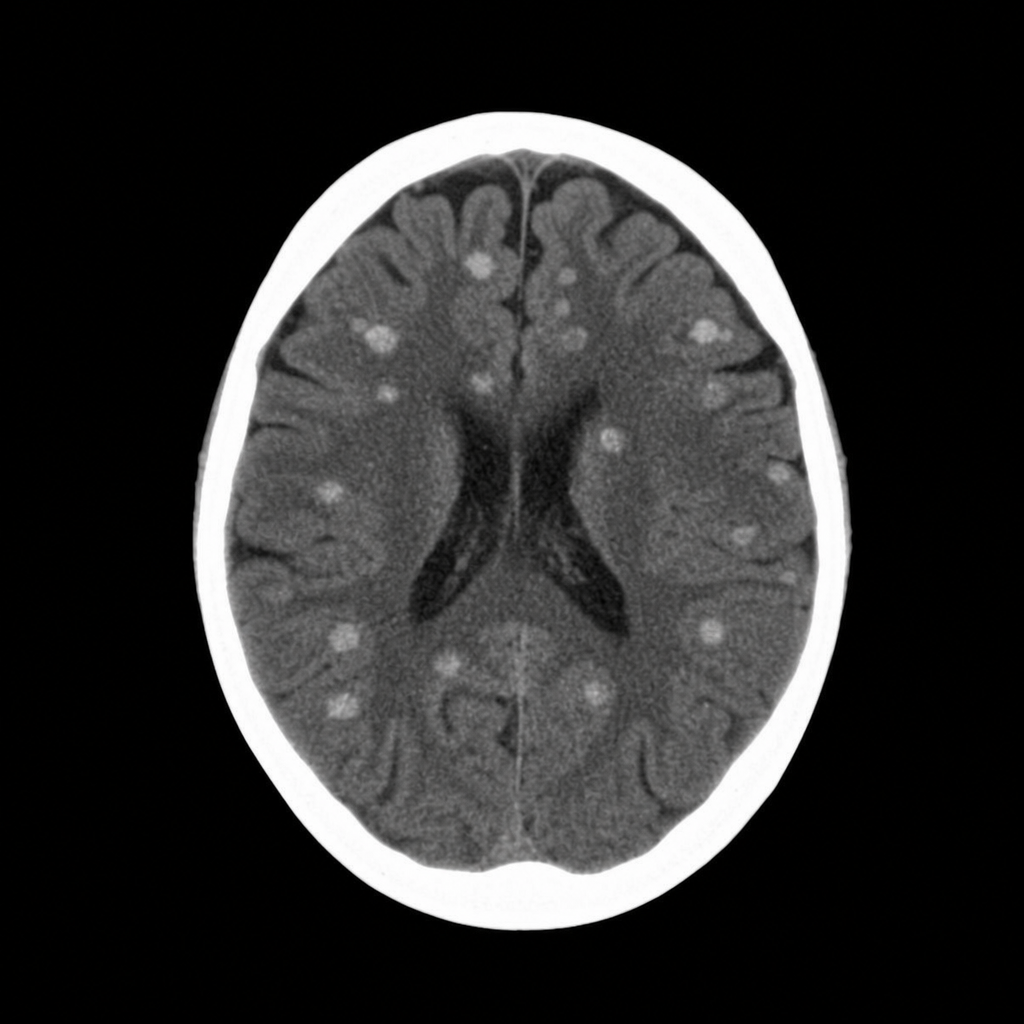
A 12-year-old boy presents with seizures that have been difficult to control with medication. A CT scan was performed. What is the most likely diagnosis?
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app