
Neuroradiology — MCQs

On this page
A cystic lesion with calcification is noted in the suprasellar region. What is the most likely diagnosis?
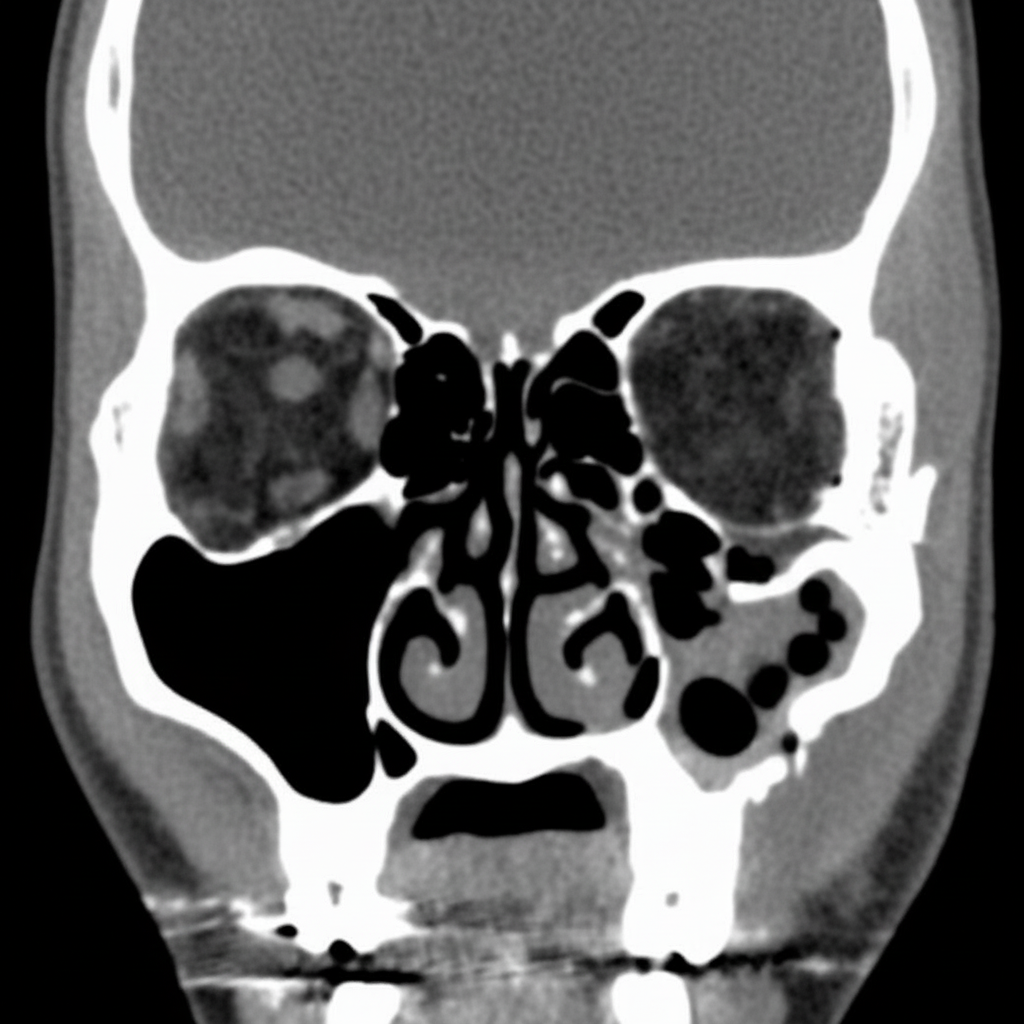
Based upon this coronal CT view of the face in a 25-year-old man with eye pain, what is the MOST likely diagnosis?
Soap bubble calcification is a feature of which condition?
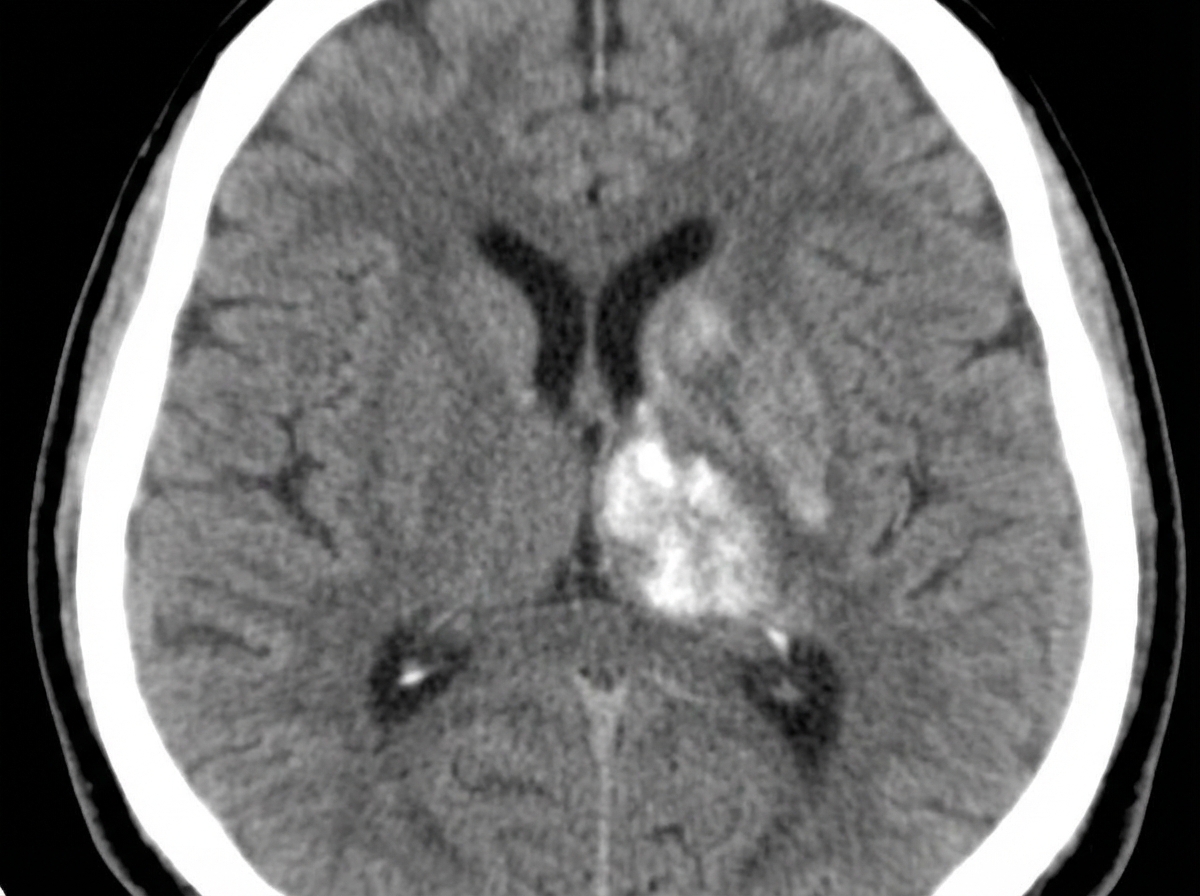
A hypertensive patient was admitted with right hemiplegia. A plain CT scan shows what?
Basal exudates, infarcts, and hydrocephalus are findings observed in brain imaging studies. What is the most likely diagnosis?
What is the most common cause of intracranial calcification?
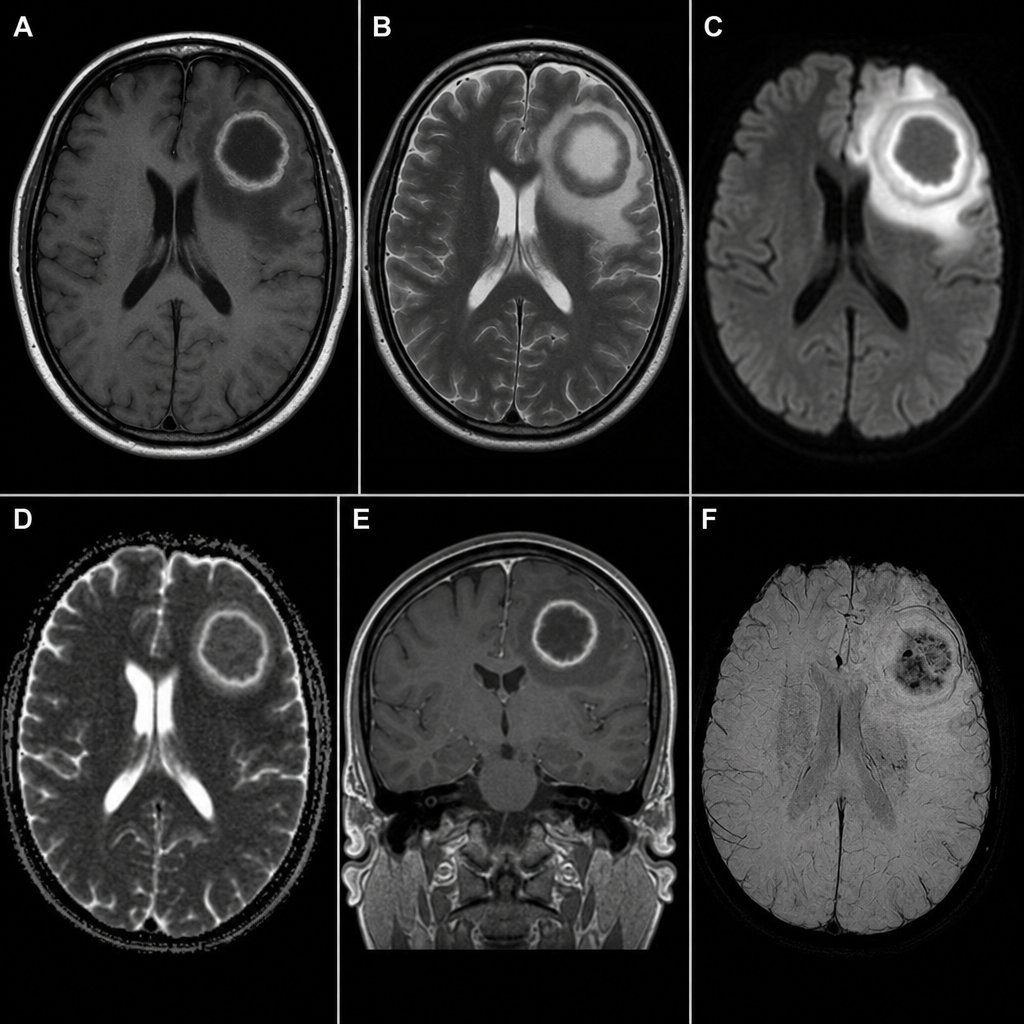
An 80-year-old male presents with a 5-day history of high-grade fever, cognitive decline, and behavioral disturbances. There is no history of travel or contact with TB patients. NCCT head revealed a hypodense lesion with edema in the left frontal lobe. MRI was performed and demonstrated a ring-enhancing lesion with central DWI hyperintensity and corresponding low ADC signal (restricted diffusion), confirming viscous pus within the cavity. What is the most likely diagnosis?
Compression of the carotid artery by a Glomus jugulare tumor is diagnosed by which imaging modality?
Which imaging modality can help to study CSF dynamics?
A dumbbell tumor is a characteristic feature of which of the following neoplasms?
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app