
Neuroradiology — MCQs

On this page
All are X-ray findings of retinoblastoma except?
What is the best imaging investigation for parameningeal rhabdomyosarcoma?
In cerebral infarct, maximum enhancement on a CT scan is typically seen after how many days?
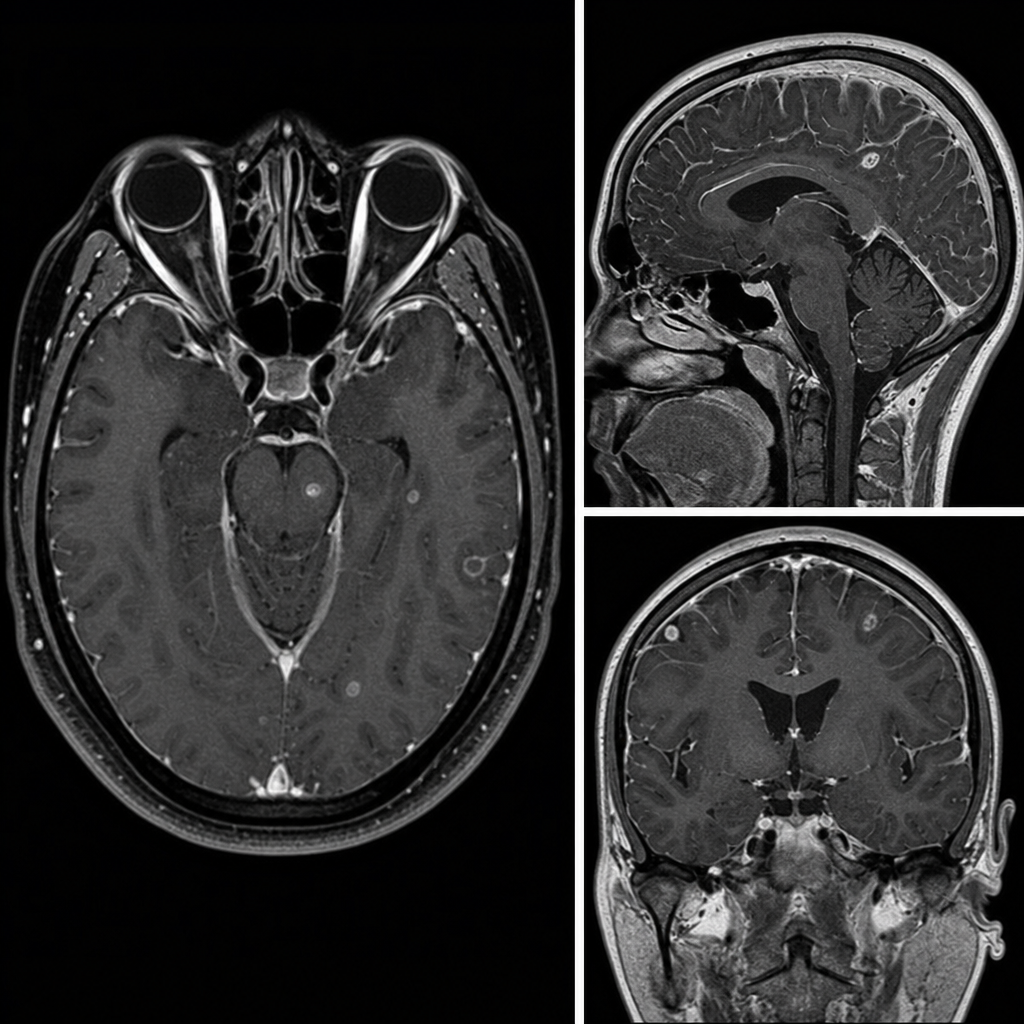
A patient with advanced HIV (CD4 count < 100) presents with headache and blurred vision for 15 days, and neck rigidity on examination. An MRI was performed. What is the most likely diagnosis?
Central T2 hypo intensity is a characteristic imaging feature of which of the following conditions?
A patient on warfarin presents with right-sided hemiplegia. What is the initial investigation of choice?
CT scan is complementary to MRI in which of the following conditions?
A 64-year-old man presents with headache and left-sided upper extremity weakness. The MRI findings suggest that this is a glioblastoma multiforme. This is because the tumor exhibits which of the following characteristics?
What is the characteristic CT scan finding of an extradural hematoma?
Feeding a nidus is characteristic of which of the following?
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app