
Neuroradiology — MCQs

On this page
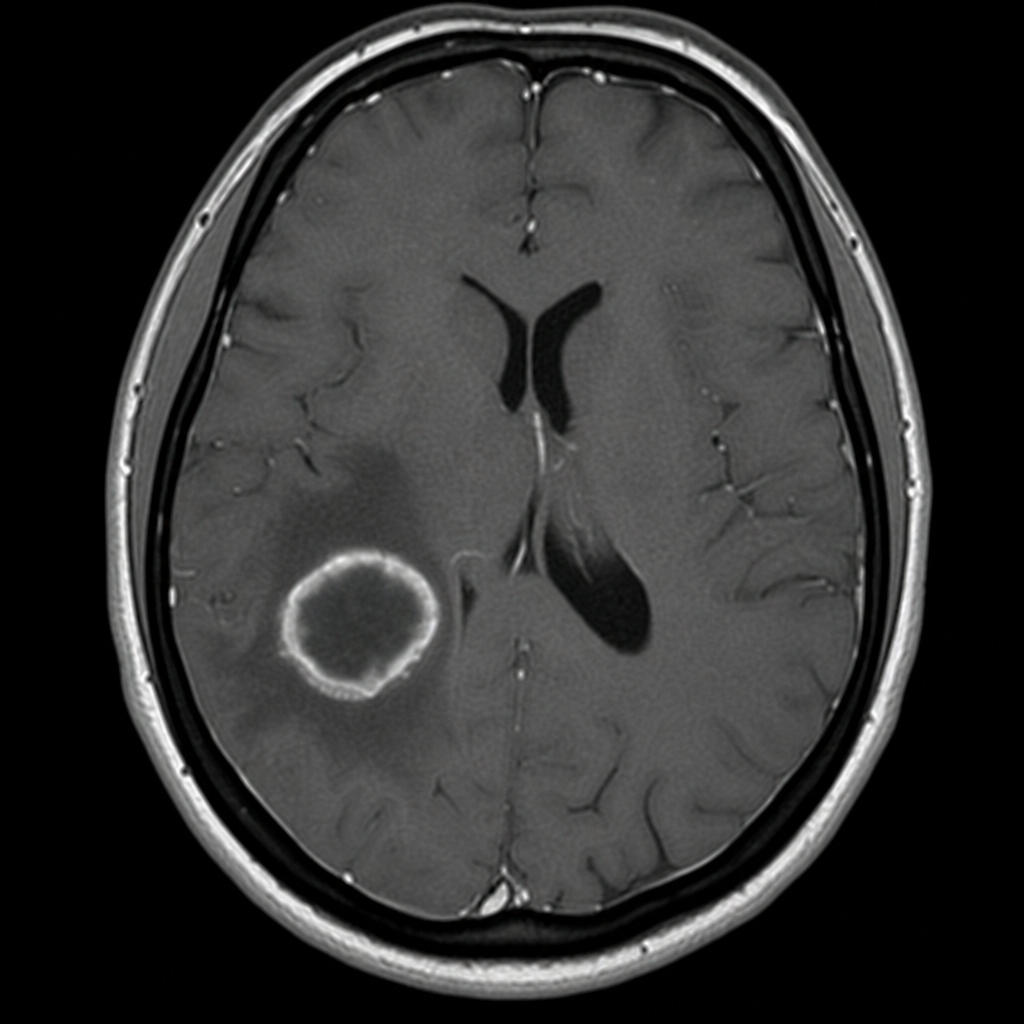
A 64-year-old man presents with headache and left-sided upper extremity weakness. The MRI of the brain is shown. What does the MRI exhibit?
Intracranial calcification is best diagnosed by?
Which of the following is NOT a typical finding of neurocysticercosis on CT scan?
What is the best imaging modality for Pelizaeus-Merzbacher disease?
Tigroid white matter is characteristically seen on MR spectroscopy in which of the following conditions?
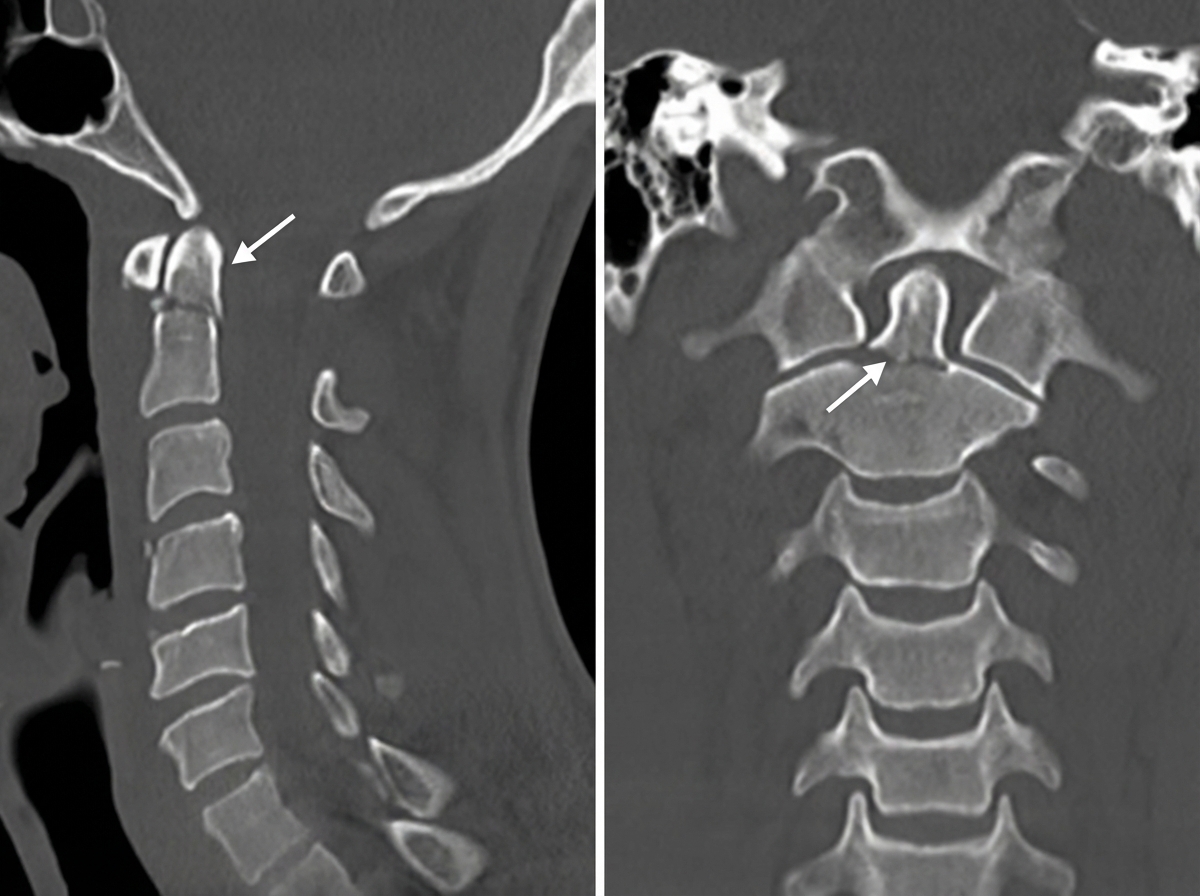
A CT scan of the neck is shown below with an arrow pointing towards the upper cervical vertebrae. What does the arrow most likely indicate?
The salt and pepper effect in MRI of the salivary gland is characteristic of which condition?
Which of the following is not a cause of communicating hydrocephalus?
A biconvex hyperdense shadow on a non-contrast CT scan is typically seen in which of the following conditions?
Boomerang ventricle is a feature of?
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app