
Neuroradiology — MCQs

On this page
What is the primary use of T2-weighted imaging in MRI?
In which condition is the 'Eye of the Tiger' appearance typically observed?
Hummingbird sign in brain MRI is seen in ?

What is the most sensitive investigation for diffuse axonal injury?
Who is credited with the development of cerebral angiography?
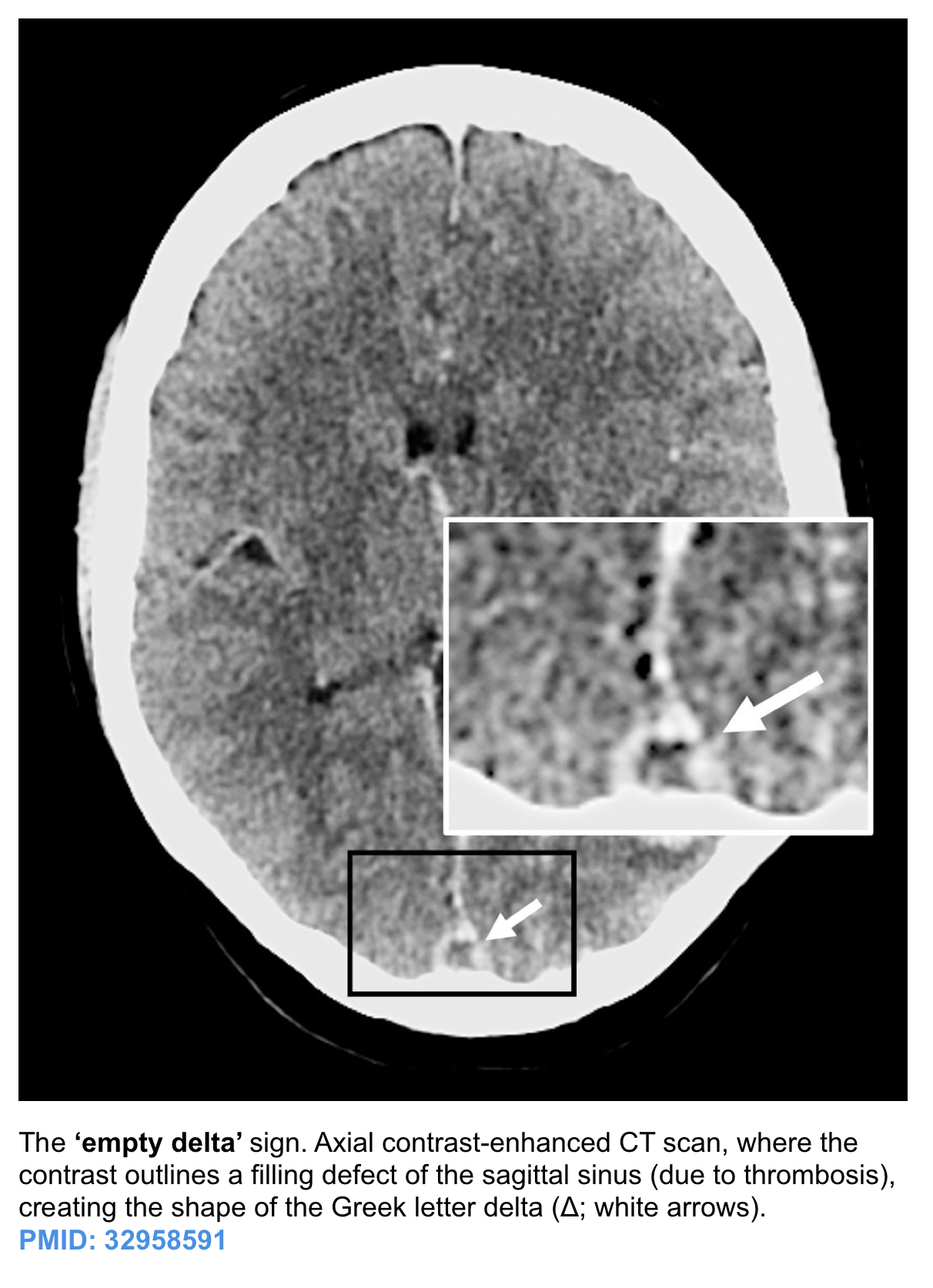
Presence of delta sign on contrast enhanced CT scan suggests presence of?
Identify the condition based on the provided image.
Identify the condition in the image below?
Tigroid pattern on MRI is seen in -
Epidural hematoma on CT scan shows which of the following?
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app