
Neuroradiology — MCQs

On this page
Which imaging modality is most sensitive for detecting early ischemic stroke?
Which of the following lesions is typically hypodense on a non-contrast CT scan?
Which imaging modality is considered the best for evaluating spinal cord compression and soft tissue abnormalities?
A 6-year-old child presents with a severe headache and vomiting. An MRI shows a cystic lesion in the cerebellum with an enhancing mural nodule. What is the likely diagnosis?
In evaluating a patient with suspected multiple sclerosis, which of the following findings would typically be seen on MRI?
A 45-year-old male patient presents with a sudden severe headache, nuchal rigidity, and loss of consciousness. A CT scan shows hyperdensity in the subarachnoid spaces. What is the next best investigation?
Which imaging modality is most appropriate for evaluating a suspected acoustic neuroma?
A 35-year-old female presents with a history of seizures and headaches. An MRI shows a well-defined cystic lesion with an enhancing mural nodule in the temporal lobe. What is the most likely diagnosis?
How does cerebrospinal fluid (CSF) appear on T1 and T2 weighted MRI images?
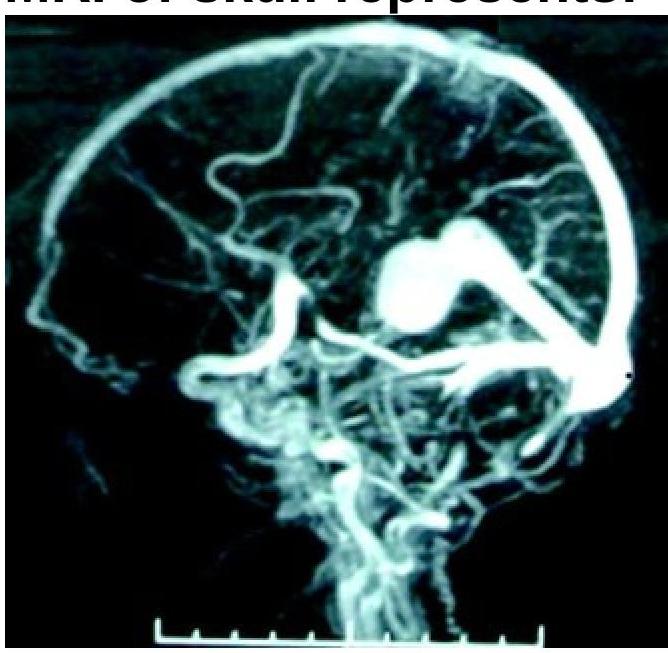
What condition is shown in the MR angiogram of the skull?
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app