
Neuroradiology — MCQs

On this page
Which of the following conditions typically presents with spinal cord edema on MRI?
What is the imaging modality of choice for determining the etiology of subarachnoid hemorrhage?
Tear-drop appearance on a PNS x-ray is seen in?

Which of the following tumors shows a radiological sign called "pneumosinus dilatans"?
Absent swallow tail sign is seen in which of the following conditions?
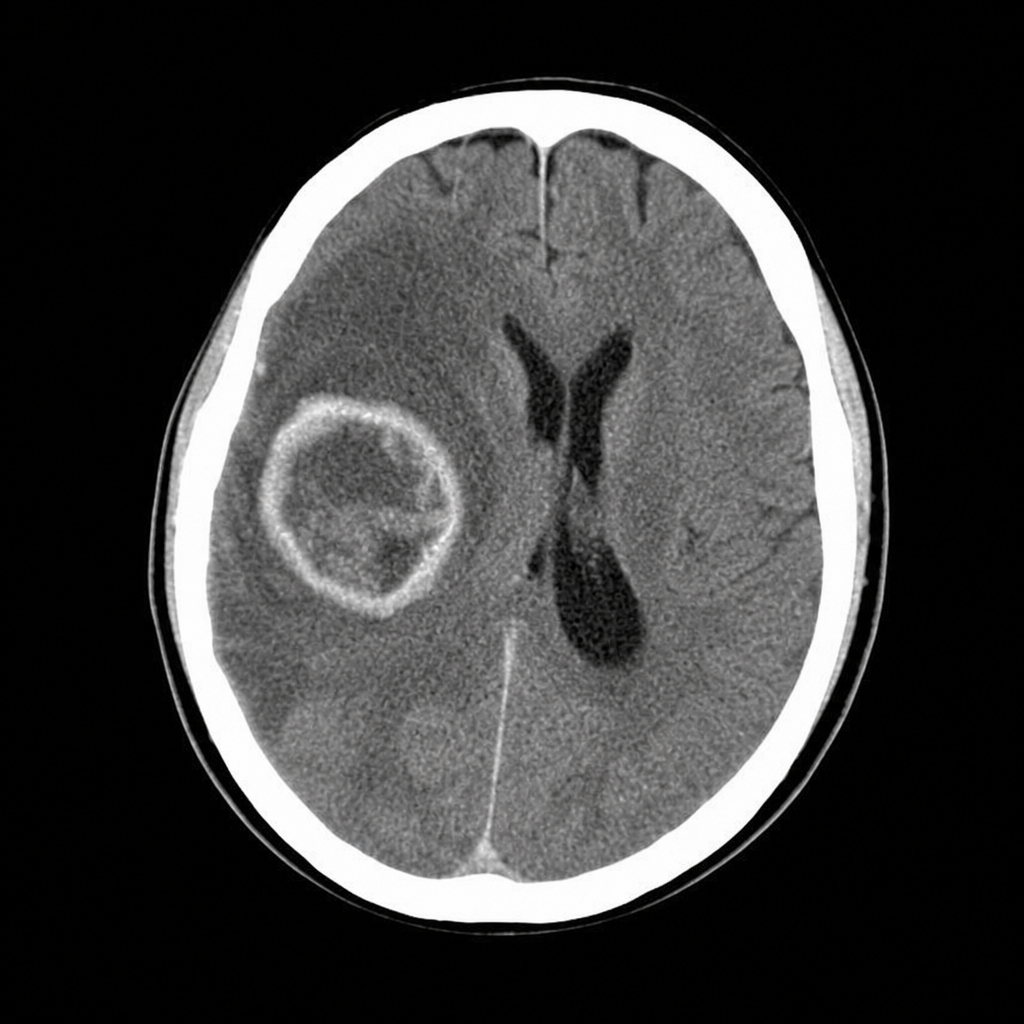
A 63-year-old man complains of worsening headache and left-sided weakness. MRI with diffusion-weighted imaging shows an irregular, thick-walled infiltrative ring-enhancing mass in the right cerebral hemisphere with surrounding vasogenic edema and no restricted diffusion within the lesion core. Based on these findings, the most likely diagnosis is:
Which condition is associated with a 'wine glass' appearance on T2-weighted MRI of the brain?
Widened neural foramina are frequently seen in:
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app