
Neuroradiology — MCQs

On this page
What are the characteristic imaging findings in Alzheimer's disease?
Which of the following conditions is characterized by bracket calcification?
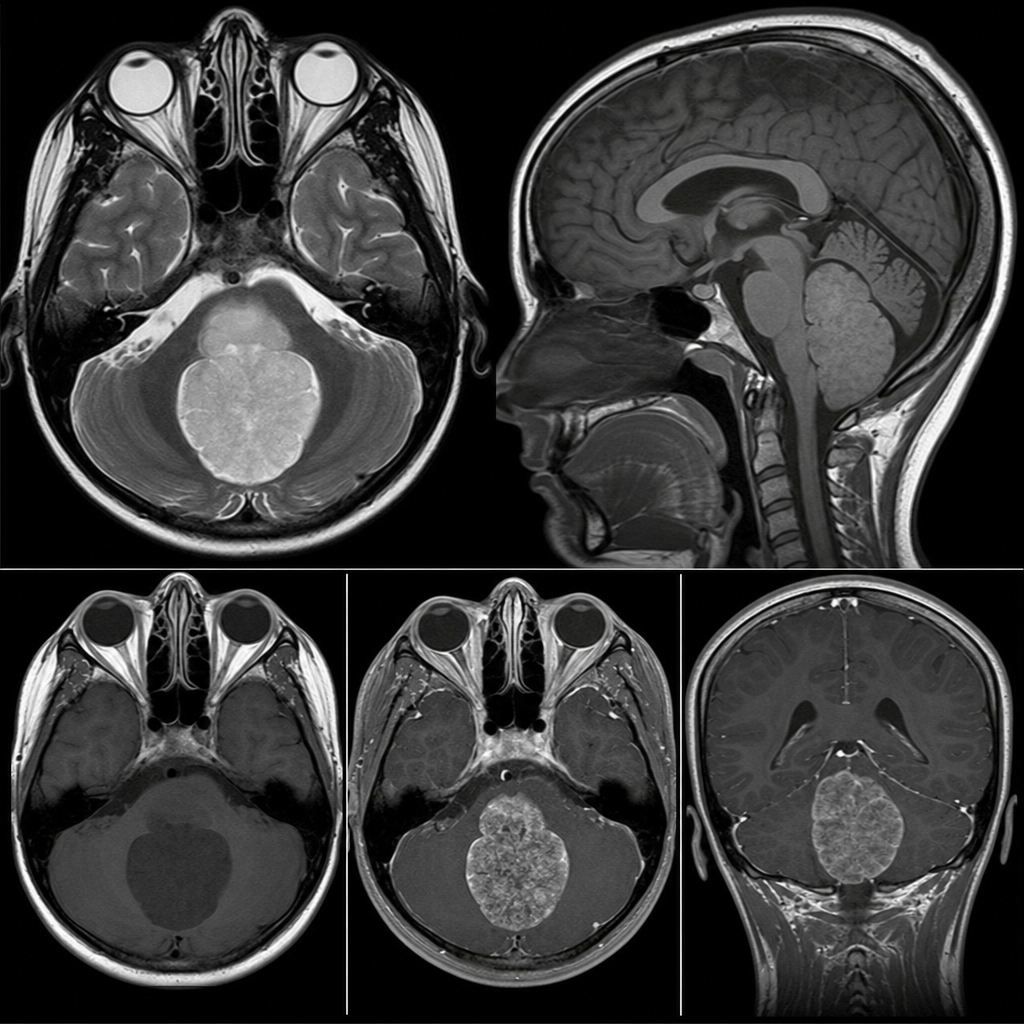
A 10-year-old male patient presents with a 20-day history of headache and vomiting. Examination reveals an ataxic gait. NCCT shows a fourth ventricular mass causing obstructive hydrocephalus. CE-MRI is performed to characterize the lesion. What is the most probable diagnosis?
Which MRI sequence is known as Tractography?
Which vessels are typically catheterized during carotid angiography?
What is the investigation of choice for acute stroke?
A 25-year-old male presents to the emergency department following an accident with symptoms of headache and paralysis. A CT scan reveals subarachnoid hemorrhage. What is the next investigation of choice?
A 12-year-old boy presents with a 6-month history of progressive intellectual decline, behavioral changes, and myoclonic jerks. CT brain shows diffuse cortical atrophy with periventricular white matter hypodensity. Which of the following viral infections is the most likely underlying cause?
A male child presents with hyperintensities on T2-weighted MRI in the bilateral frontal lobes. What is the most probable diagnosis?
A 5-year-old child presents with a cystic lesion with an enhancing mural nodule in the cerebellar hemisphere on brain MRI. What is the most likely diagnosis?
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app