
Neuroradiology — MCQs

On this page
Investigation of choice for screening of proximal internal carotid artery stenosis is :
Which of the following conditions is least likely to cause posterior scalloping of the vertebrae?
Which condition is characterized by the 'Eye of the Tiger' sign on MRI?
Best method of detection of a retained glass intraocular foreign body is
What is the investigation of choice in a patient with traumatic paraplegia?
Which of the following brain structures does not contribute to the Mickey Mouse sign on axial brain imaging?
Which of the following is not a sign of increased intracranial tension?
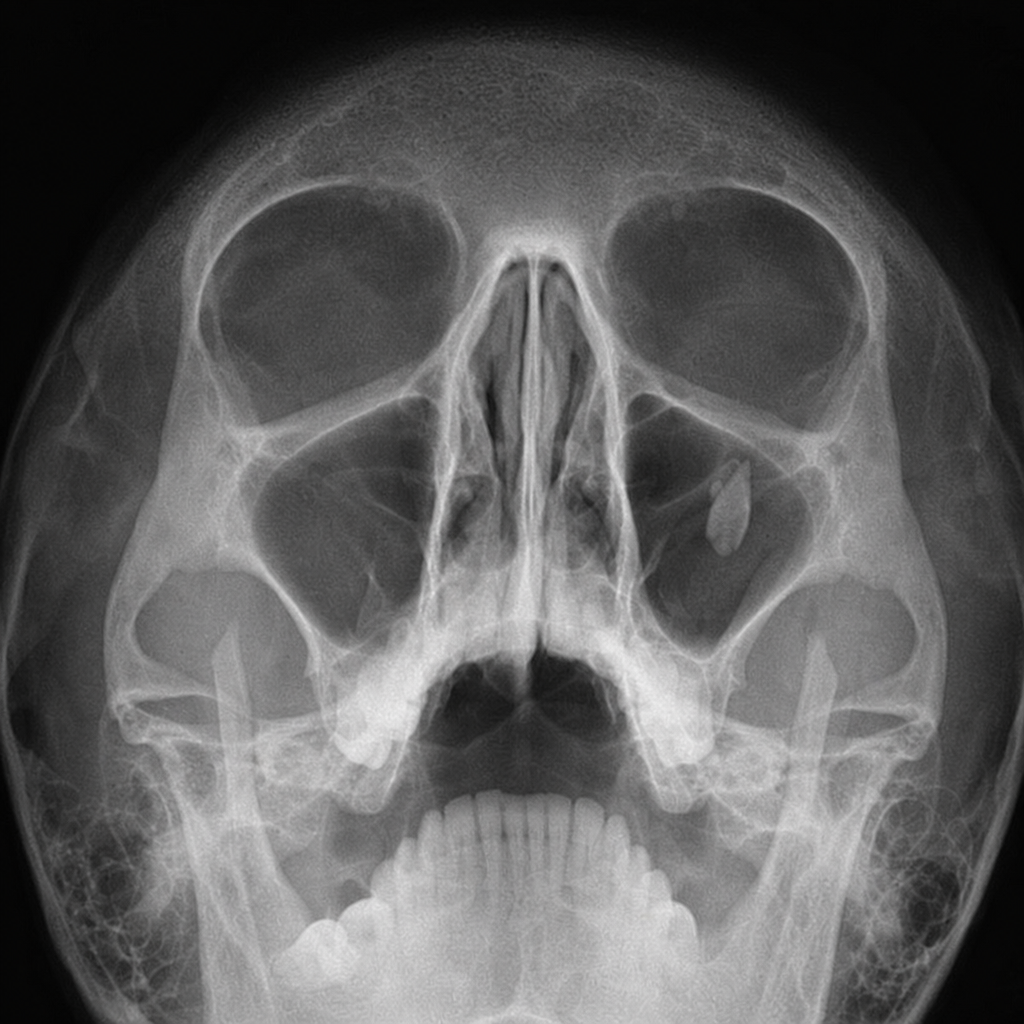
Tear drop sign on X-ray of the paranasal sinuses is seen in
What is the most common cause of periventricular calcification?
In which of the following diseases is the NAA peak seen?
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app