
Neuroradiology — MCQs

On this page
A 35-year-old female presents with a history of seizures and headaches. An MRI shows a well-defined cystic lesion with an enhancing mural nodule in the temporal lobe. What is the most likely diagnosis?
Identify the condition based on the provided image.
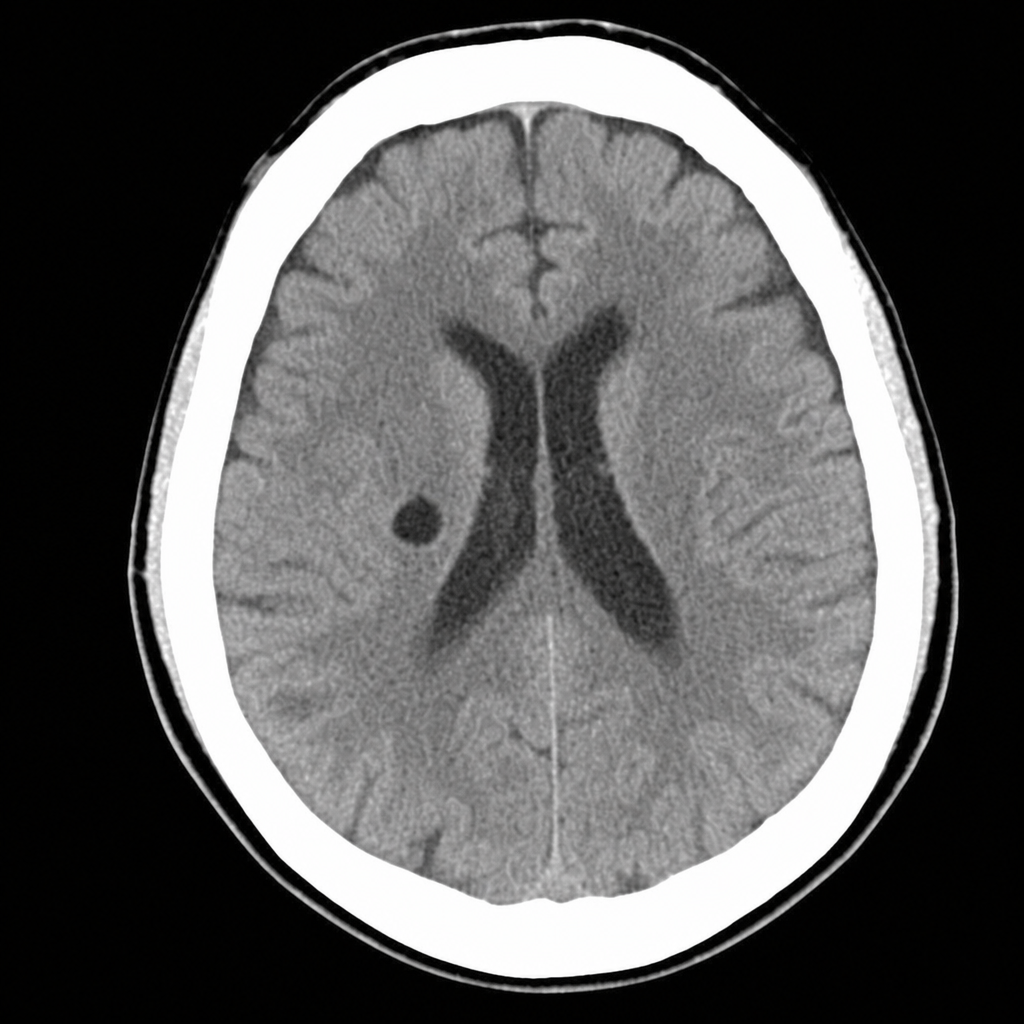
A 65-year-old patient with long-standing hypertension develops sudden left-sided pure motor weakness without aphasia, neglect, visual-field loss, or other cortical signs. The noncontrast head CT shown demonstrates a hypodense infarct involving the right basal ganglia and adjacent internal-capsular region, without acute hemorrhage. Which stroke subtype best explains these findings?
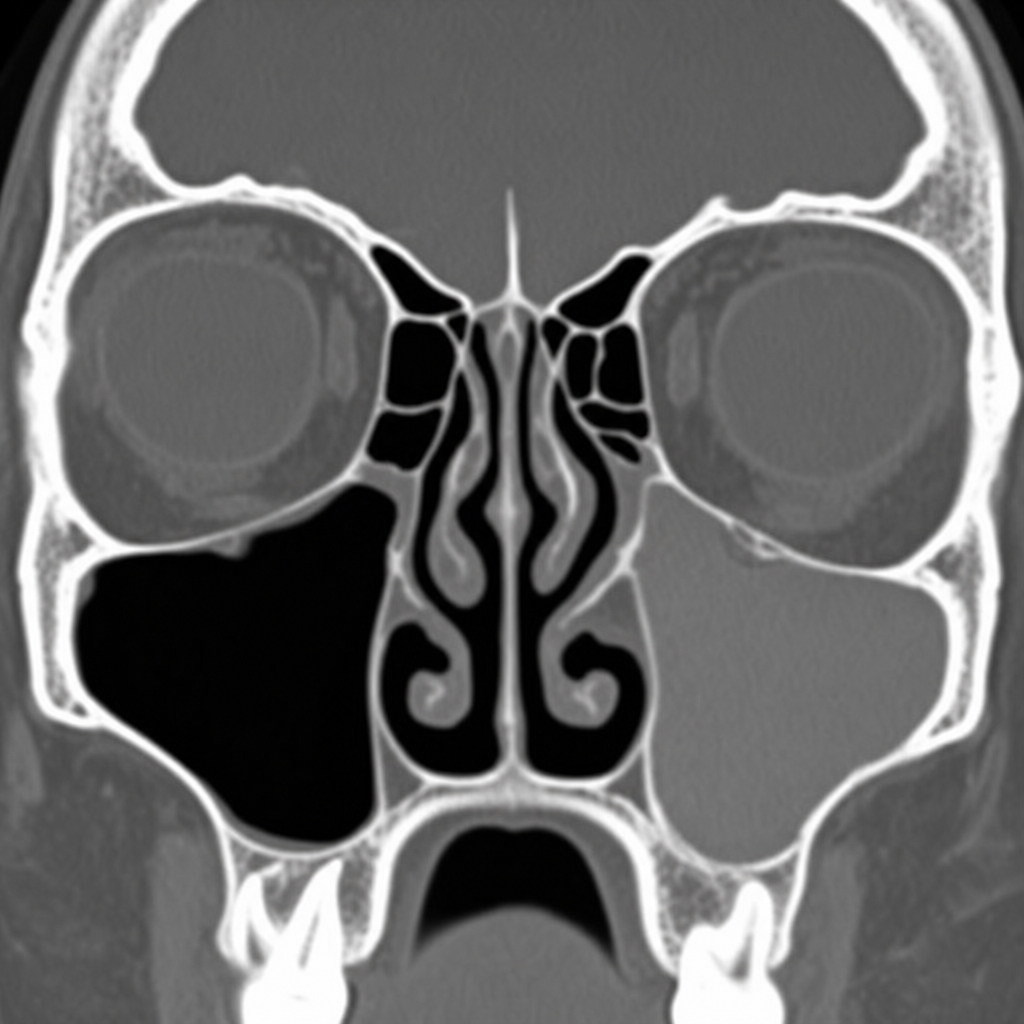
A CT image of the left maxillary sinus shows heterogeneous opacification with a central hyperdense region surrounded by a peripheral rim of lower attenuation soft tissue. The patient has a history of allergic rhinitis. What is the most likely finding in this CT image?
Stenver's view is used for -
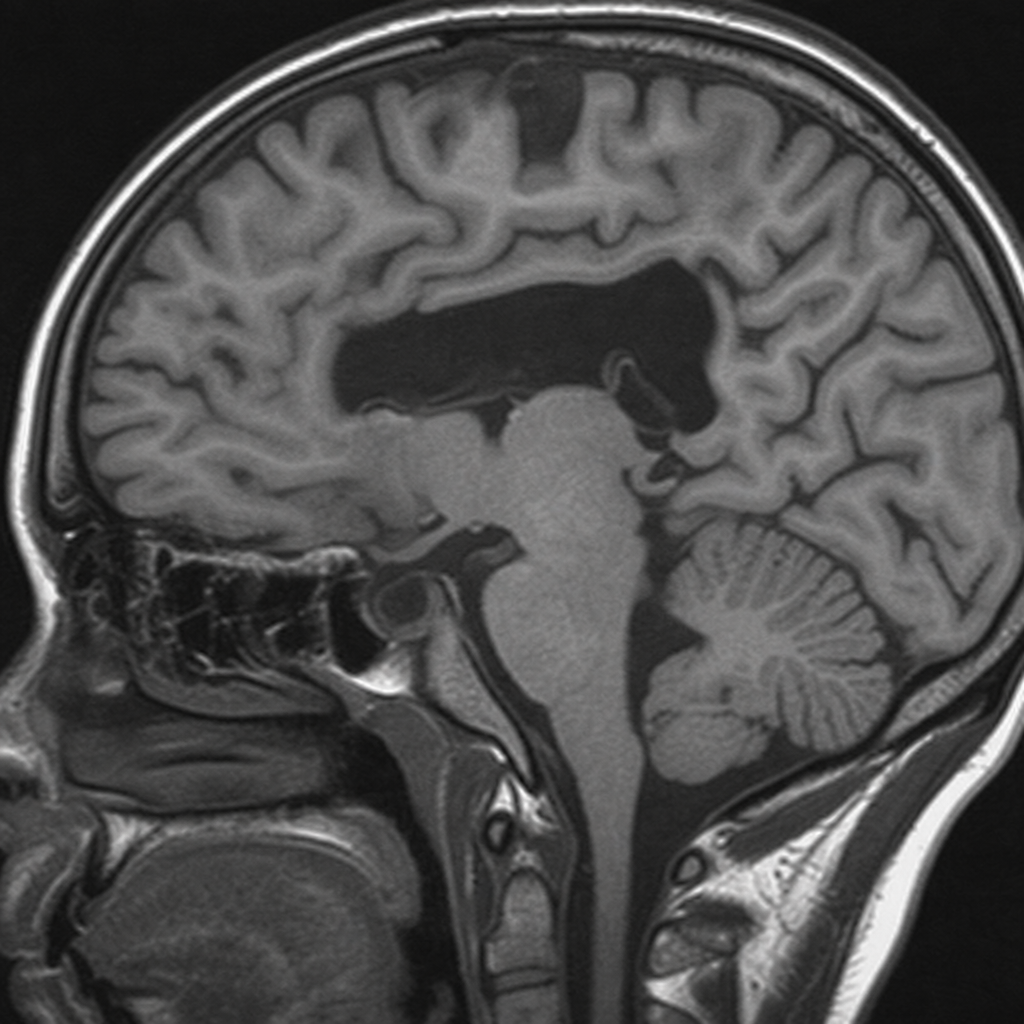
How does cerebrospinal fluid (CSF) appear on T1 and T2 weighted MRI images?
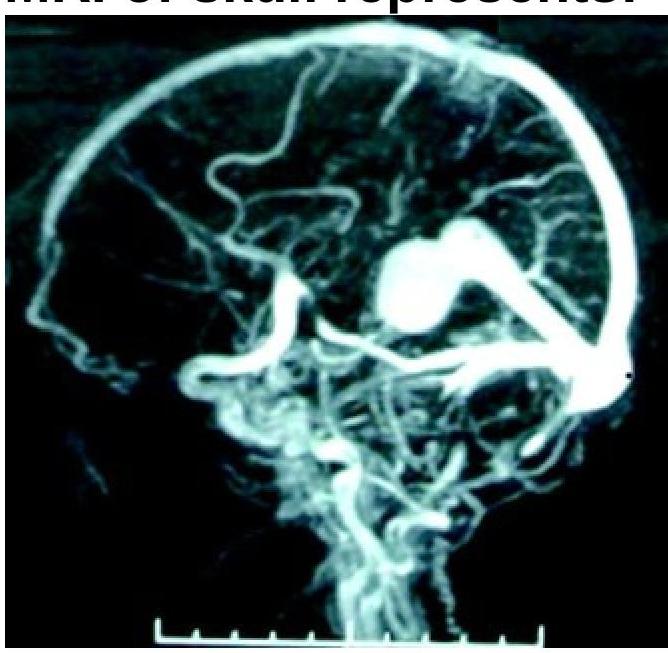
What condition is shown in the MR angiogram of the skull?
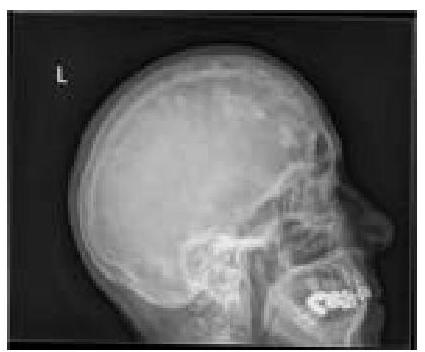
Which diagnosis is most strongly suggested by the numerous, well-circumscribed punched-out lucencies in the skull calvarium on this radiograph?
Which of the following provides excellent details about the chemodectomas?
What is the most sensitive investigation for diffuse axonal injury?
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app