
Neuroradiology — MCQs

On this page
A young adult presents with proptosis and pain in eye after 4 days of trauma to eye. Chemosis, conjunctival congestion and extraocular muscle palsy with inability to move eye are seen.Investigation of choice -
Which one of the following is the most preferred route to perform cerebral angiography?
Investigation of choice for lumbar prolapsed disc -
The investigation of choice for vestibular schwannoma is
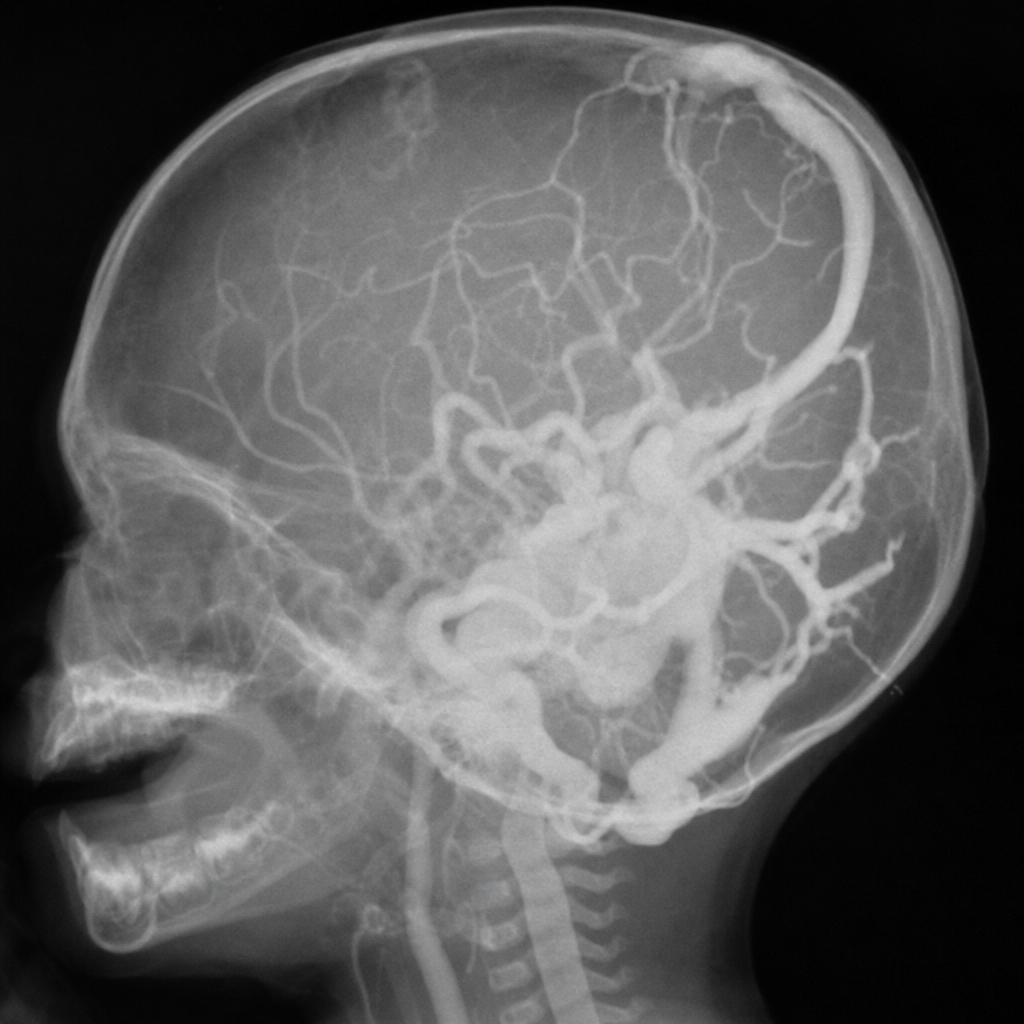
New born male baby presented with congestive heart failure. On examination enlarged fontanelles, a loud cranial bruit and following radiological finding was noted - the most likely diagnosis:
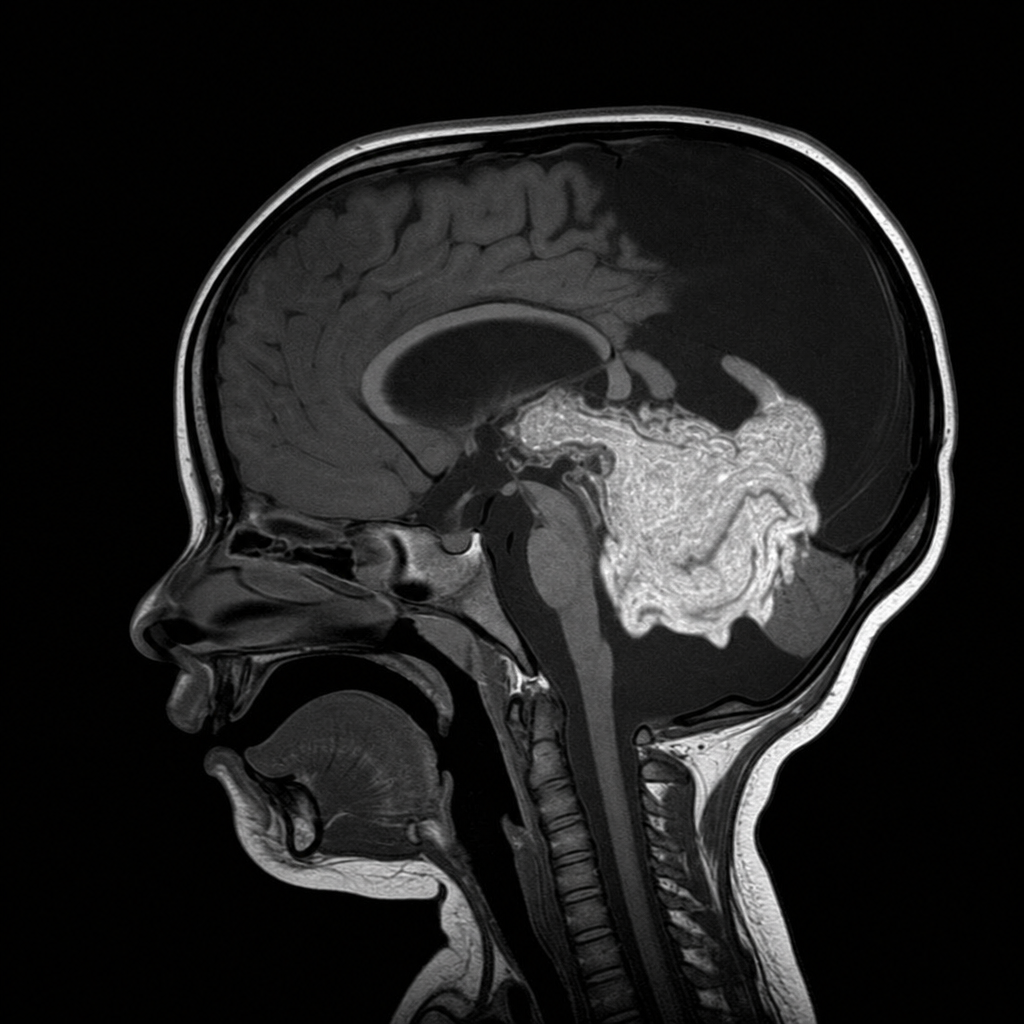
Newborn male baby presented with congestive heart failure. On examination enlarged fontanelles, a loud cranial bruit and following radiological findings were noted - the most likely diagnosis is:
Dawson's fingers are seen in -
A 45-year-old female complains of progressive lower limb weakness, spasticity, and urinary hesitancy. MRI shows an intradural enhancing mass lesion in the spinal cord. MOST likely diagnosis is:
Corpus callosum involvement on MRI is usually seen in which of the following conditions?
Investigation of choice for leptomeningeal carcinomatosis:
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app