
Neuroradiology — MCQs

On this page
Investigation of choice in cerebral abscess is -
Shape of post traumatic Epidural hematoma is
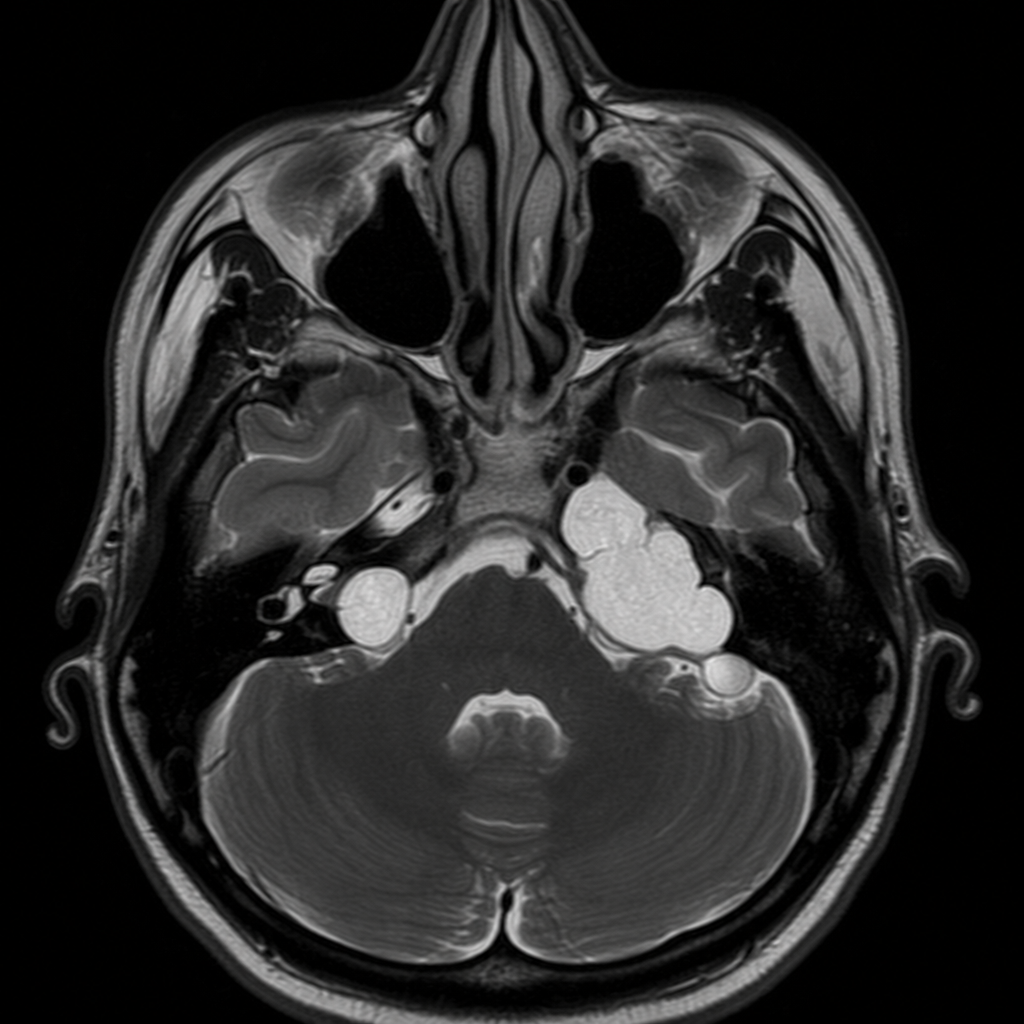
MRI done in a 28yrs old male suffering from Neurofibromatosis 2 showed ice cream cone appearance. On asking he further revealed that it began with ringing sensation in ears which progressed to balance problems and hearing loss. Which of the following is the most likely diagnosis -
First sign of hydrocephalus in children is:
A leukemia patient who has undergone multiple courses of chemotherapy develops herpes simplex encephalitis. Which of the following would you expect a CT scan of the patient's brain to show?
Which of the following is not true about non-contrast CT scan in head injury?
Banana sign seen in the fetal brain suggests ?

Shape of extradural hematoma on NCCT is?
A 32-year-old woman is evaluated in the clinic for symptoms of polyuria and polydipsia. She has no significant past medical history and her only medication is the oral contraceptive pill. Her physical examination is entirely normal. Urine and serum biochemistry investigations are suggestive of central diabetes insipidus (DI). Which of the following is the most likely finding on magnetic resonance imaging (MRI) of the brain?
A middle aged female presents with prolonged history of back pain followed by slowly progressive weakness of both lower limbs, spasticity and recent onset difficulty in micturation. On neurological examination there is evidence of dorsal myelopathy. MRI scan of spine shows a well-defined mid-dorsal intradural homogenous contrast enhancing mass lesion. The likely diagnosis is:
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app