
Neuroradiology — MCQs

On this page
A 40-year-old male presents with a history of headaches, fever, and new-onset seizures. An MRI of the brain is performed, revealing a ring-enhancing lesion with central restricted diffusion on diffusion-weighted imaging (DWI). What is the most likely diagnosis?
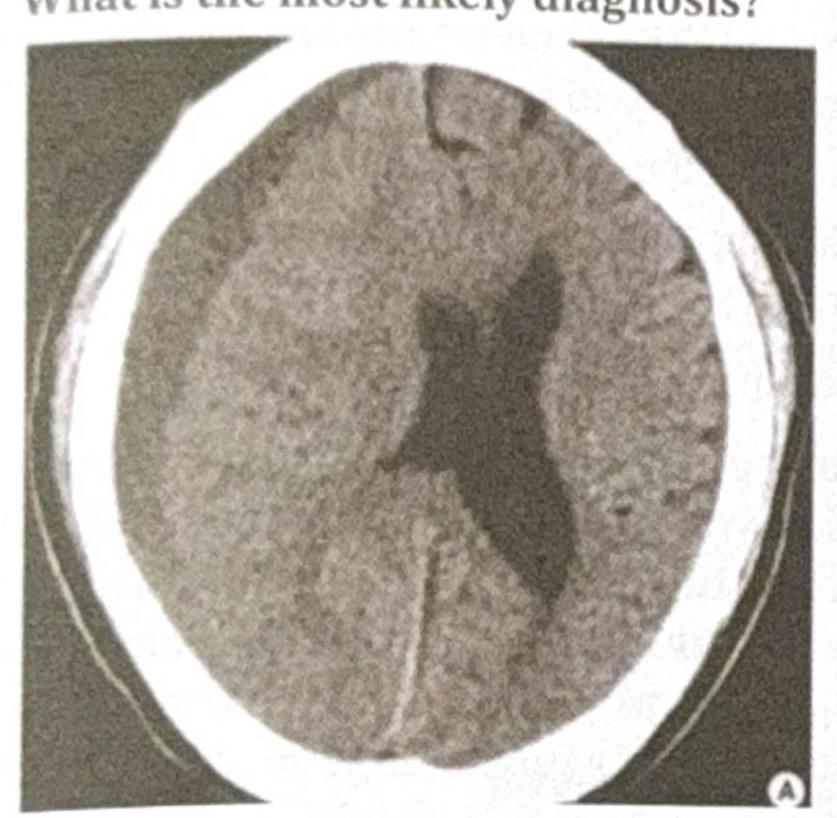
An 80-year-old male with a history of frequent falls presents with progressive headache, confusion, and mild hemiparesis over the past few weeks. A CT scan of the head is performed, and the image provided shows a crescent-shaped, hypodense collection over the left cerebral hemisphere with a slight midline shift. What is the most likely diagnosis?
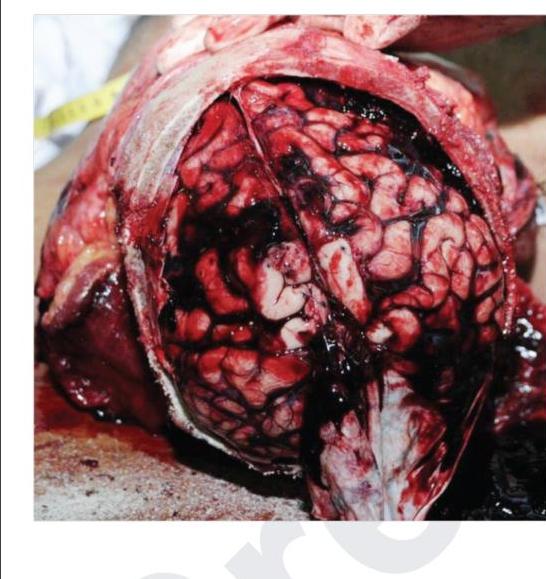
Bleeding as shown in the image is due to which of the following vessels?
A cerebral angiogram shows stenosis of the terminal internal carotid arteries with an abnormal network of collateral vessels. Which finding is most characteristic of moyamoya syndrome?
An MRI brain shows 'molar tooth sign' in the posterior fossa. This radiological finding is pathognomonic for which condition?
A brain MRI shows 'hot cross bun' sign in pons. Which additional finding would best support the diagnosis of multiple system atrophy?
An MRI brain shows 'pencil shavings' appearance in the corpus callosum. Which additional finding would best support the diagnosis of multiple sclerosis?
What is the investigation of choice for diagnosing subarachnoid hemorrhage (SAH)?
A man presents to the emergency department with a head injury following a vehicular accident. What is the investigation of choice?
Most common cause of suprasellar enlargement with calcification in children is –
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app