
Neuroradiology — MCQs

On this page
Which peak on MR spectroscopy is seen in tuberculoma?
Deep white matter lesions with bilateral deep bright thalamic appearance are suggestive of which disease?
A 7-year-old patient presents with headache, paralysis of upward gaze, loss of light perception and accommodation, nystagmus, and failure of convergence. CT scan showed a homogenous hyperdense lesion above the sella and in the posterior part of the third ventricle. MRI showed that the lesions were homogenous and isointense on T1-weighted imaging, and isointense on T2-weighted imaging with intense contrast enhancement. What is the most likely diagnosis?
In children, increased intracranial pressure is manifested by which of the following?
An extra-axial enhancing lesion is seen on MRI. What is the most likely diagnosis?
What is the investigation of choice for cystic lesions in the brain?
Subependymal calcified nodules are seen in which of the following conditions?
CT findings in Epidural Hematoma (EDH) are typically described as?
Upstream and downstream hydrocephalus is seen in which of the following conditions?
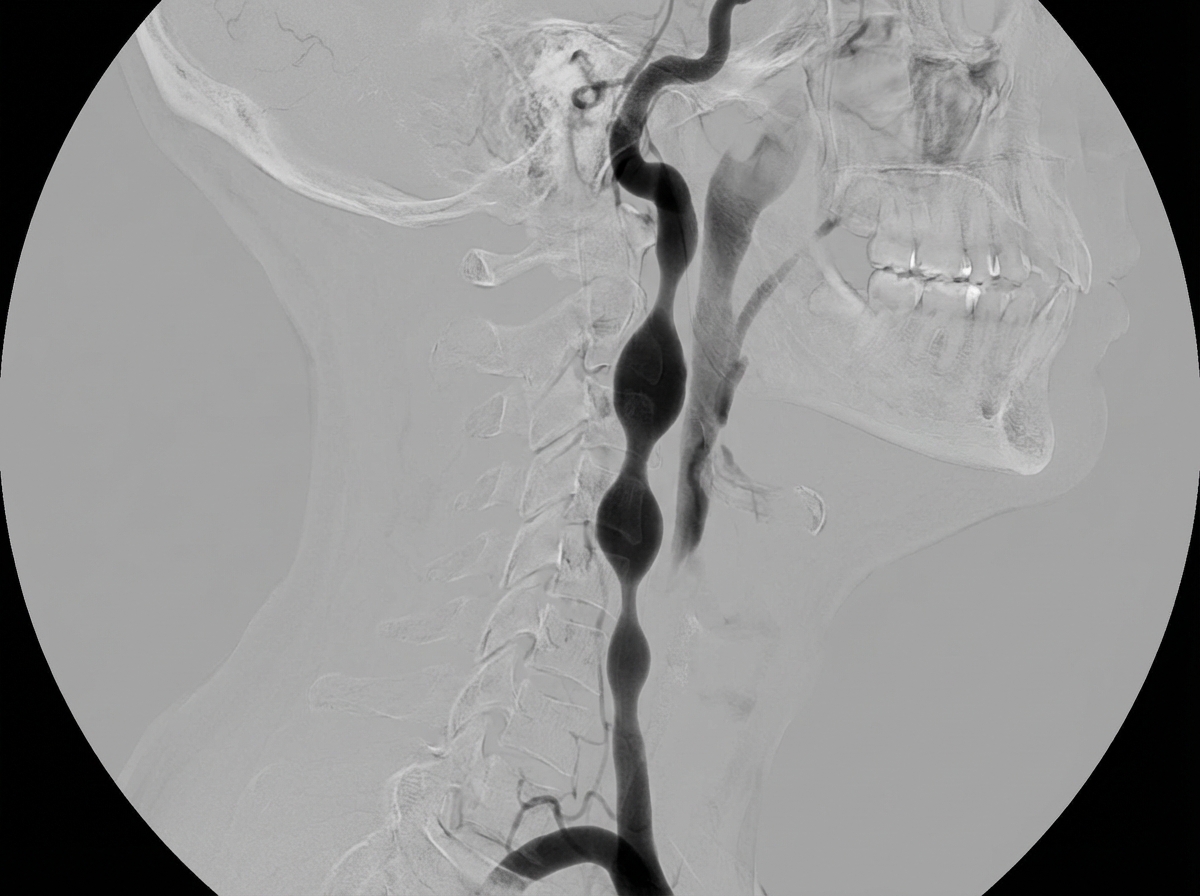
A 35-year-old female presented with a history of multiple transient ischemic attacks. What is the most likely diagnosis suggested by the given carotid angiogram?
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app