
Neuroradiology — MCQs

On this page
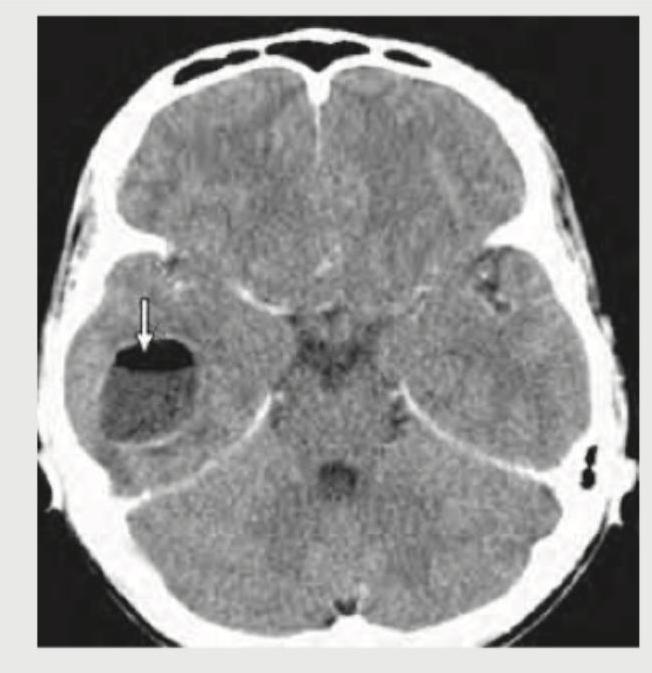
The CT head of this infant with macrocephaly shows:
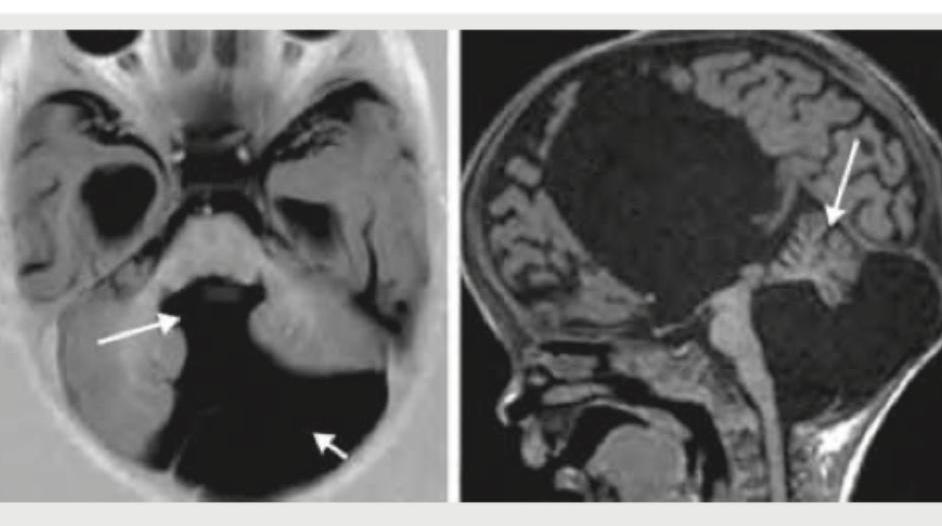
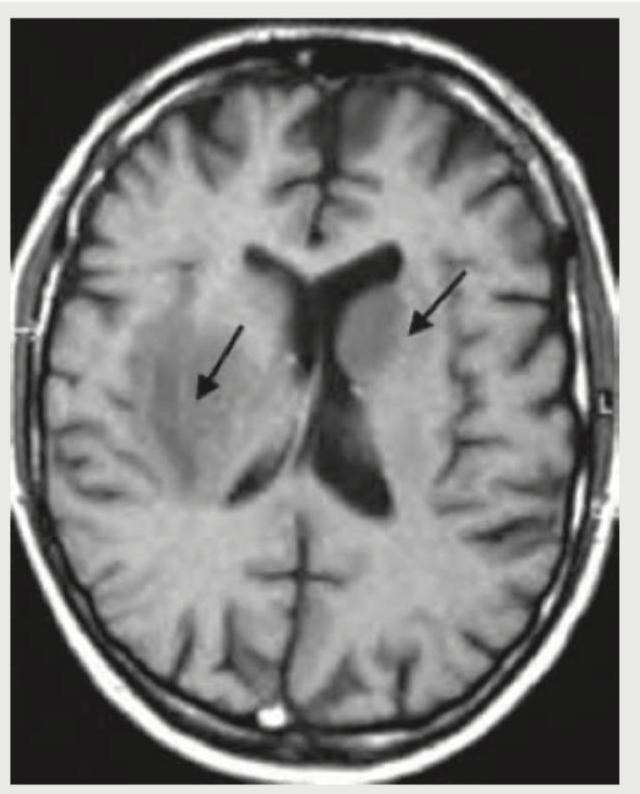
The given MRI head shows:
What is the most likely diagnosis on this CECT head?
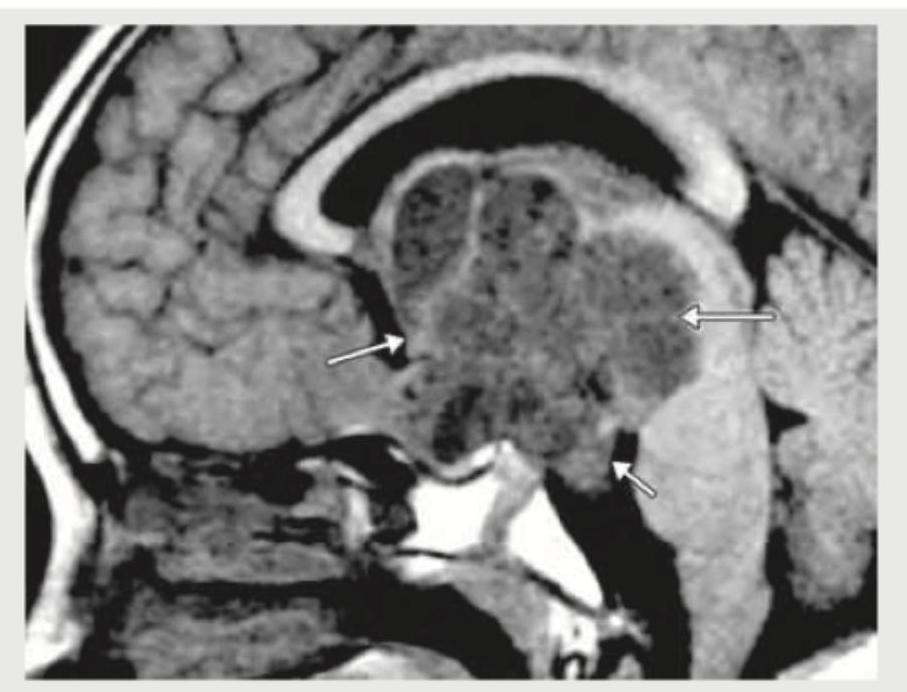
The given MRI head shows:
A 25-year-old AIDS patient who had stopped taking ART for 6 months presented with seizures and altered sensorium. MRI head of the patient shows:
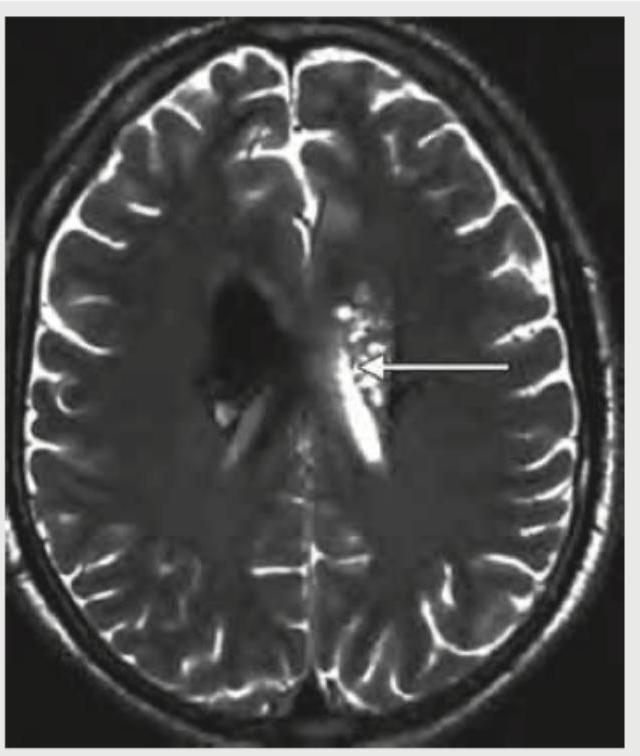
A 35-year-old immunocompromised patient presents with headache and altered sensorium. The following T2-weighted MRI head shows:
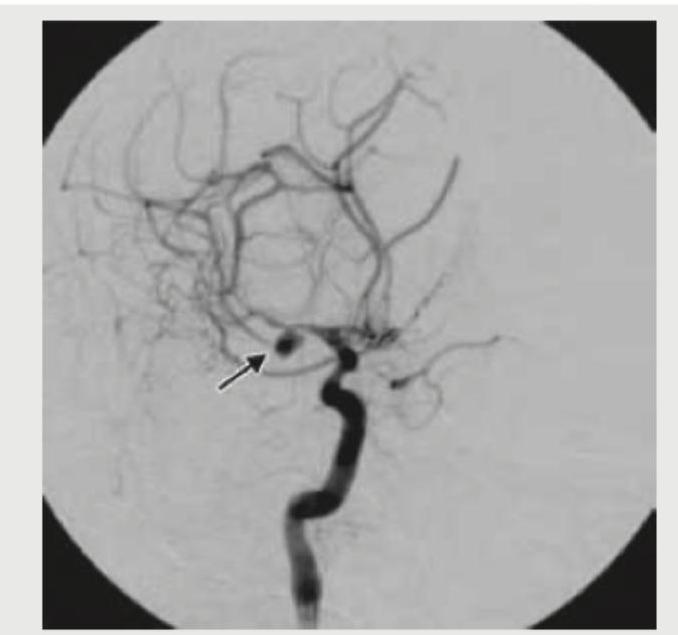
The digital subtraction angiography given below shows? (AIIMS Nov 2017)
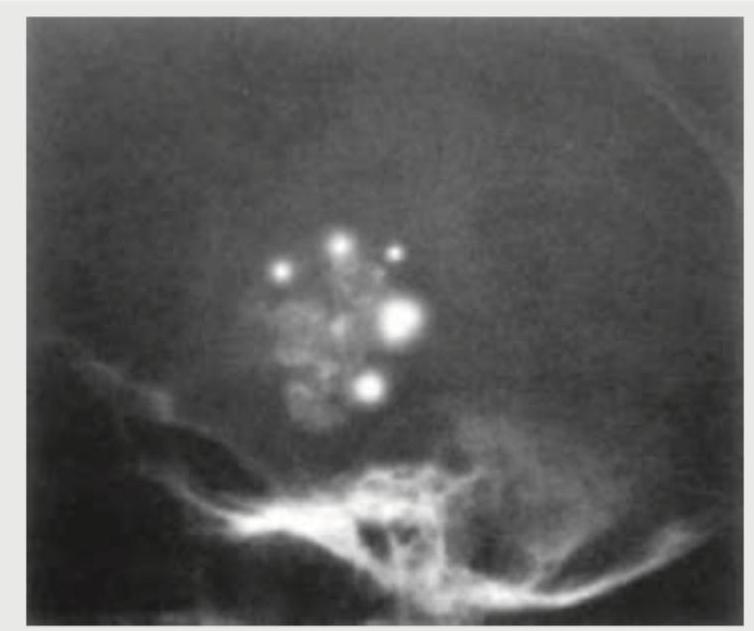
A 9-year-old female child presents with history of headache and visual disturbances. X-Ray skull is shown below. What is the possible diagnosis? (Recent NEET Pattern 2018-19)
A 55 year old male came with history of hoarseness of voice for which direct laryngoscopy was done and the lesion was biopsied to detect squamous cell carcinoma. He now requires investigation to detect extent of cartilage involvement, imaging of pre and paraglottic spaces and any extension to deep neck structures. Most appropriate investigation of choice will be:
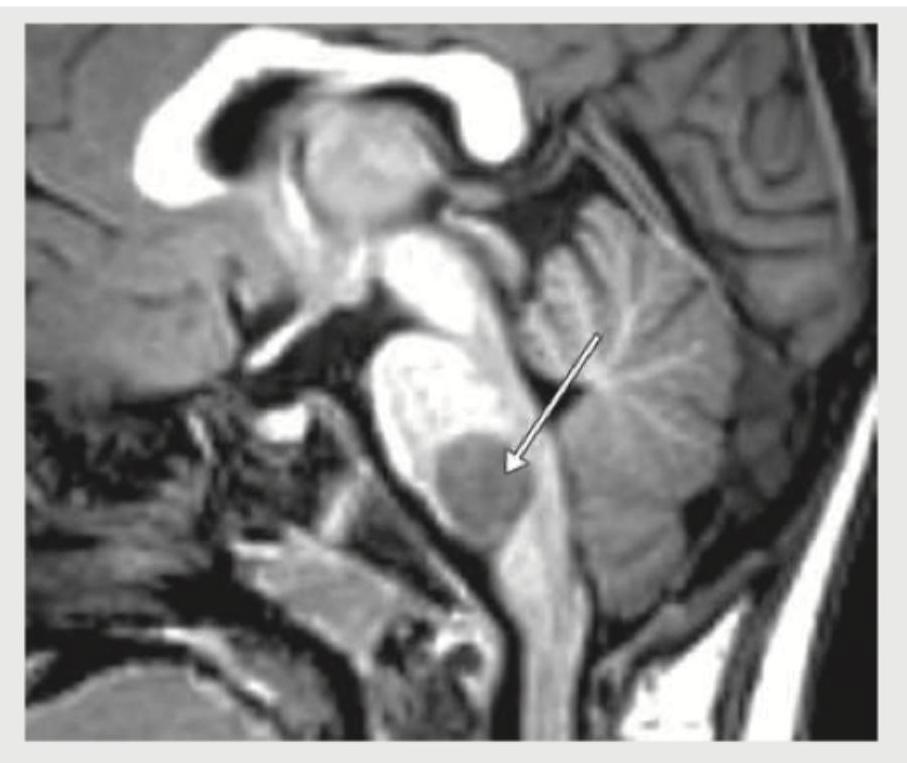
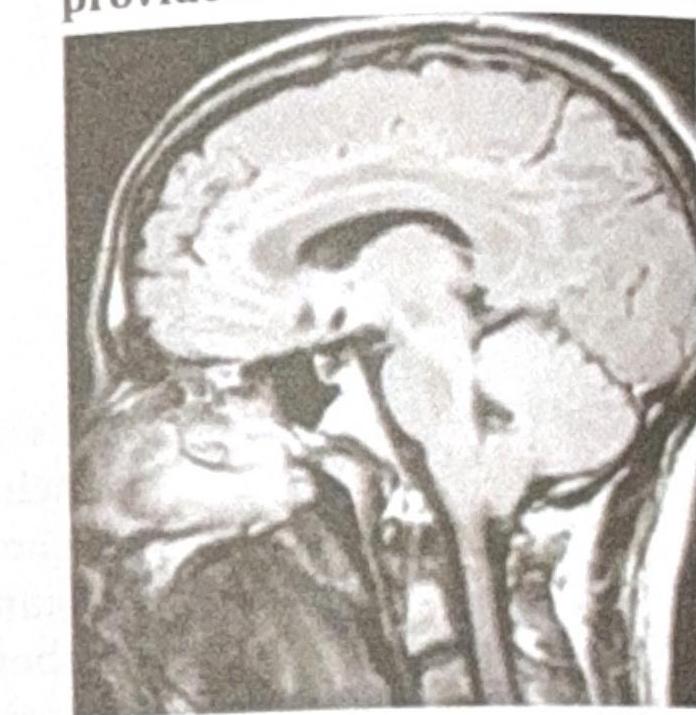
Identify the diagnosis using the MRI provided.
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app