
Neuroradiology — MCQs

On this page
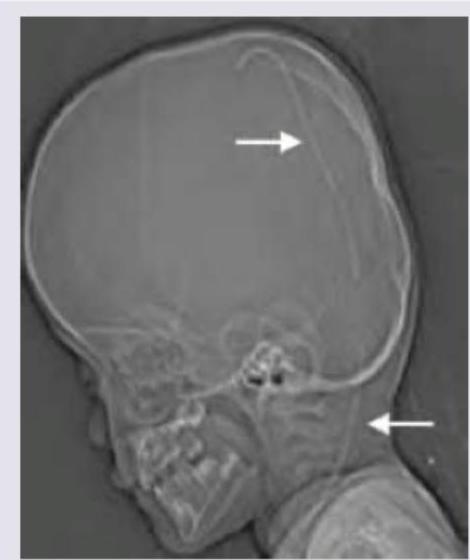
A 79-year-old male presented to the emergency department after a facial trauma. The patient had Parkinson's disease and atrial fibrillation and was on treatment with acetylsalicylic acid for AF. The image shows? (Recent NEET Pattern 2016-17)
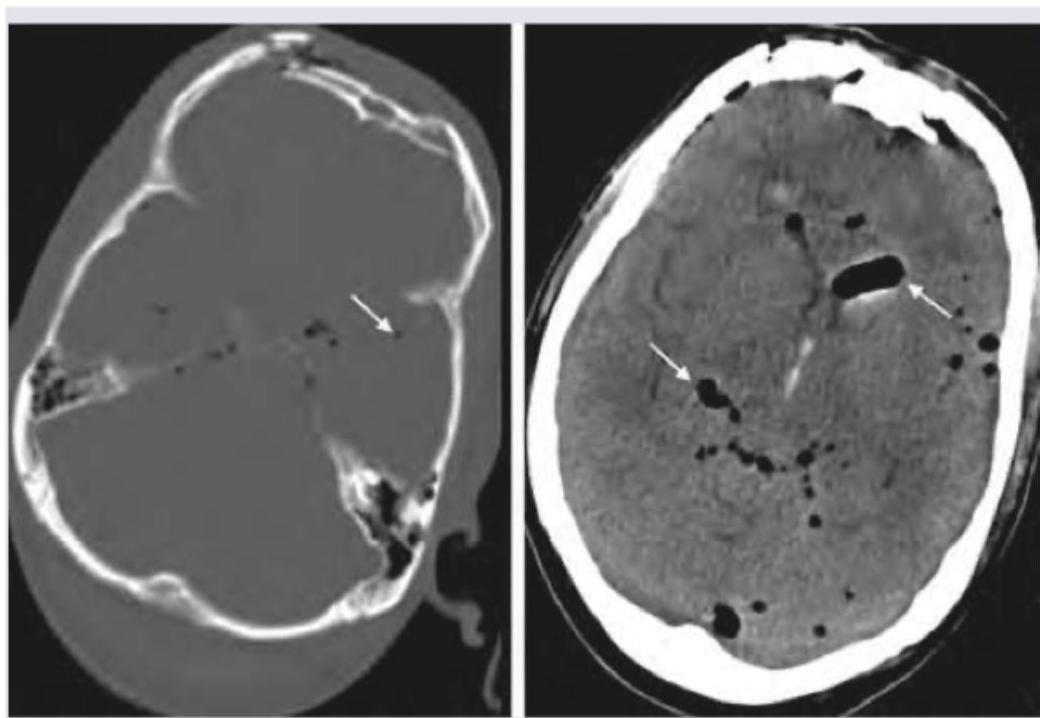
What intracranial complication is demonstrated by the frontal extra-axial hypodensity?
A 2-year-old epileptic child with developmental delay presents to emergency with fever for the last two days. NCCT shows:
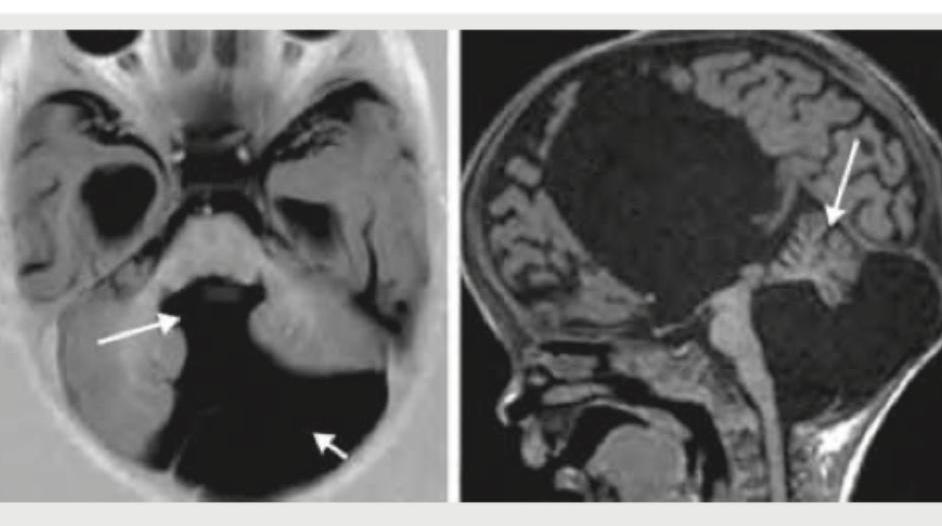
All are true about CNS malformation shown below except:
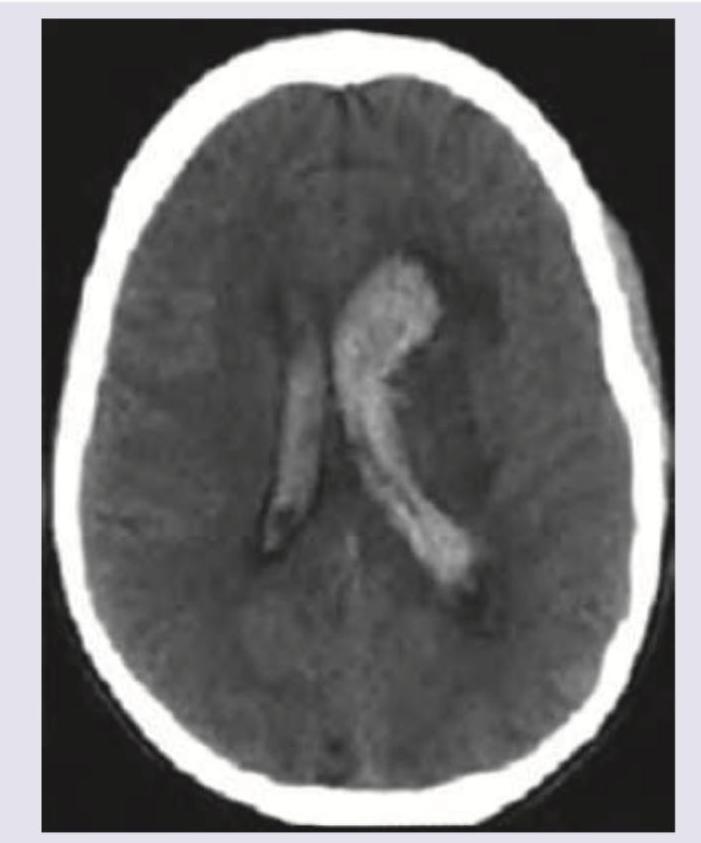
The image given below shows presence of:
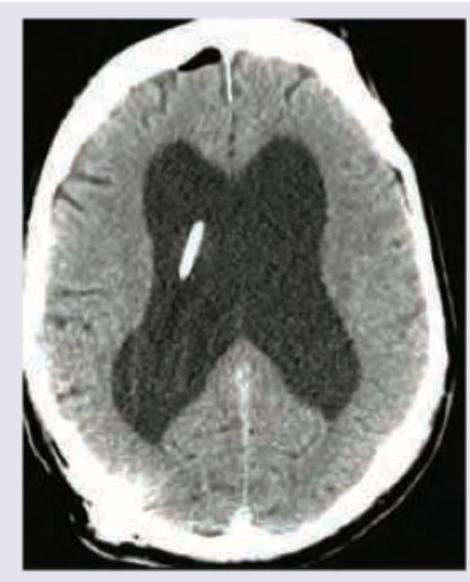
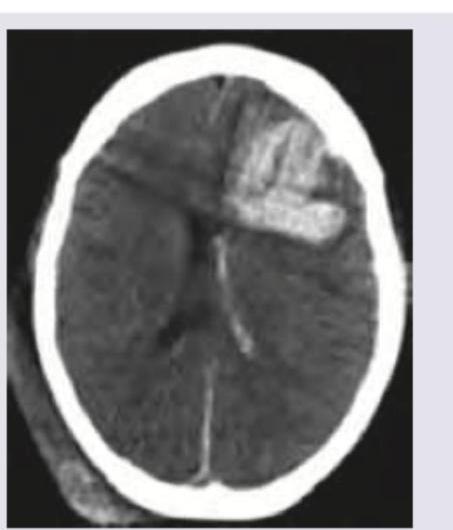
The NCCT head scan of a 45-year-old head injury patient shows:
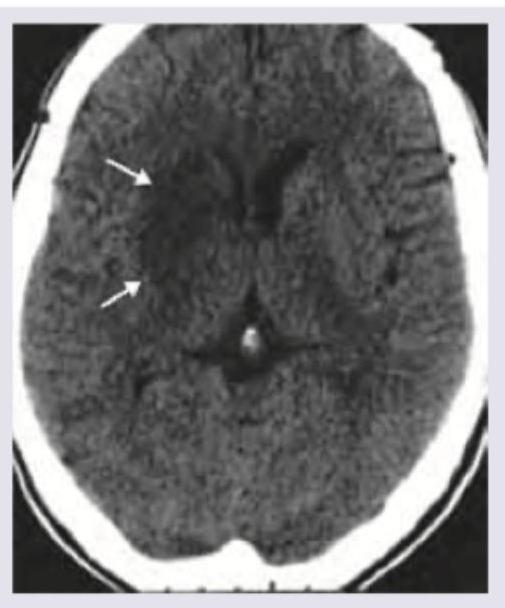
The given NCCT shows the presence of:
Which of the following is correct about the NCCT shown below? (Recent NEET Pattern 2016-17)
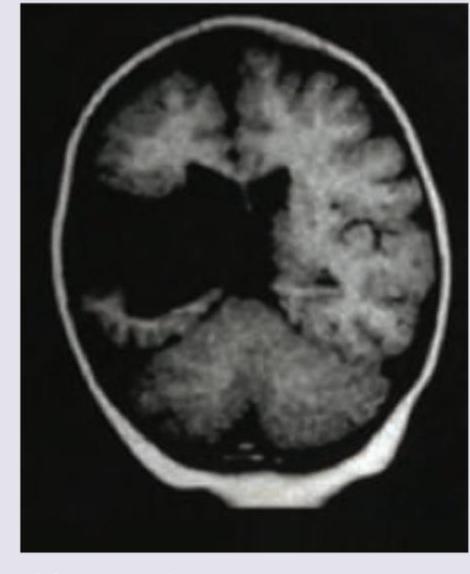
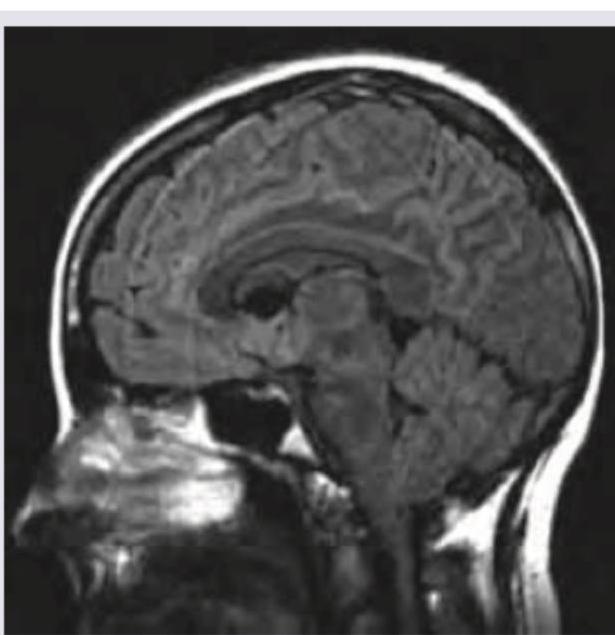
The MRI head of this infant with macrocephaly shows which of the following?

The CT head of this infant with macrocephaly shows:
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app