
Neuroradiology — MCQs

On this page
A 6-year-old boy presented with complex seizures per day in spite of an adequate 4-drug antiepileptic regimen. He had a history of repeated high-grade fever in childhood. MRI for epilepsy protocol revealed a normal brain scan. Which of the following will not be helpful for functional imaging of the brain?
MRI is the investigation of choice in all of the following except:
What is the investigation of choice for subdural hemorrhage?
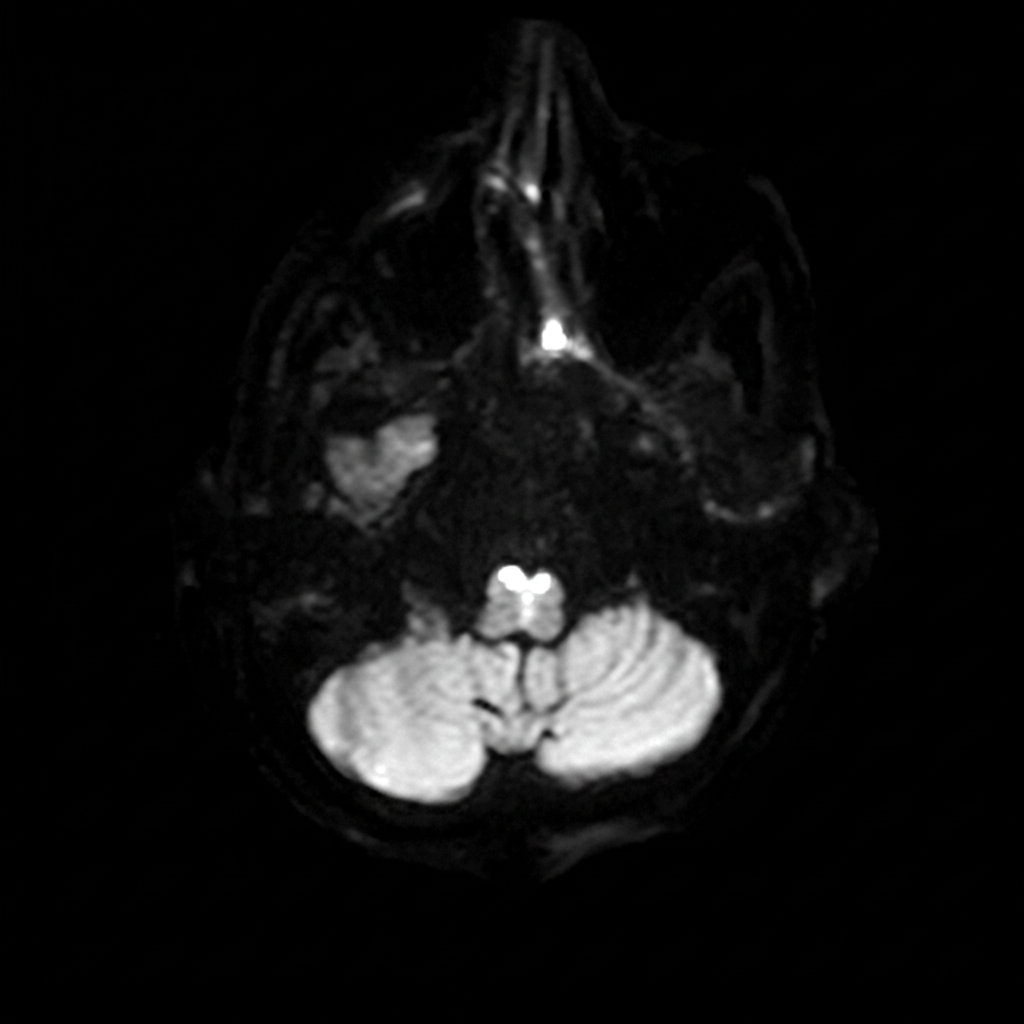
Which condition is characterized by the following sign?
Echoencephalography is most useful in detecting which of the following?
Geographic lytic lesions in the vault of the skull with bevelled edges are seen with which condition?
Mount Fuji sign is a feature of which of the following conditions?
What is the imaging tool of choice for evaluating a lacunar infarct?
A patient presents with severe headache. A CT scan of the brain reveals hyperdense areas in the right basal region, marked as 'X'. Which of the following is the most likely diagnosis?
A 30-year-old female patient involved in a road traffic accident had nausea and vomiting. She was brought unconscious to the emergency room. The NCCT brain reveals the following findings. What is the most likely diagnosis? 
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app