
Neuroradiology — MCQs

On this page
What is the investigation of choice for spinal tuberculosis?
Which of the following is NOT a characteristic feature of meningioma?
Which of the following statements about CT scan is FALSE?
"Lyre sign" is a feature of:
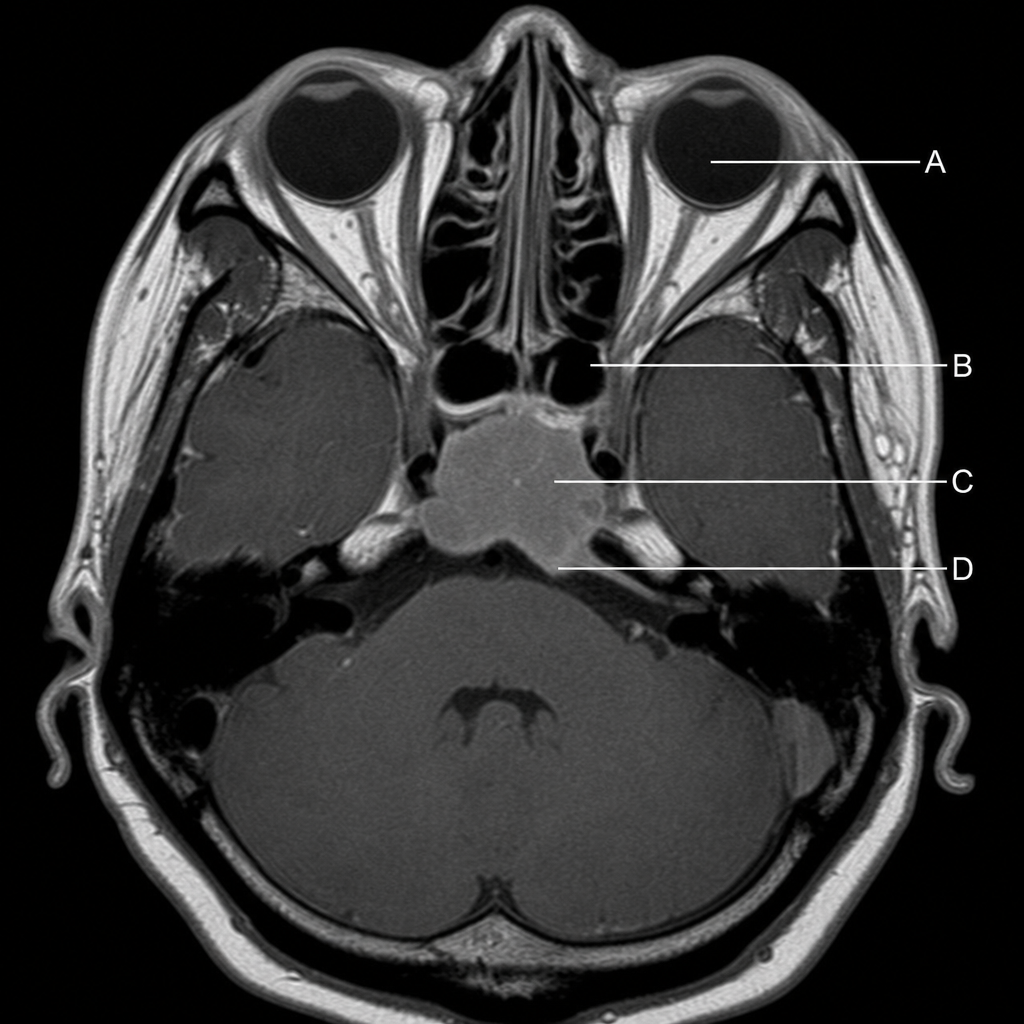
Which structure may be obliterated by a pituitary tumor, as indicated in this MRI scan showing a transaxial section through the head?
Which of the following features is a classic radiologic feature of optic nerve glioma?
Suprasellar calcification is a feature of which of the following tumors?
Which of the following signs is classic for CT scanning in Graves ophthalmopathy?
What is the earliest method for diagnosing a pituitary tumor?
Cavernous hemangioma is characterized by which of the following radiological findings?
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app