
Neuroradiology — MCQs

On this page
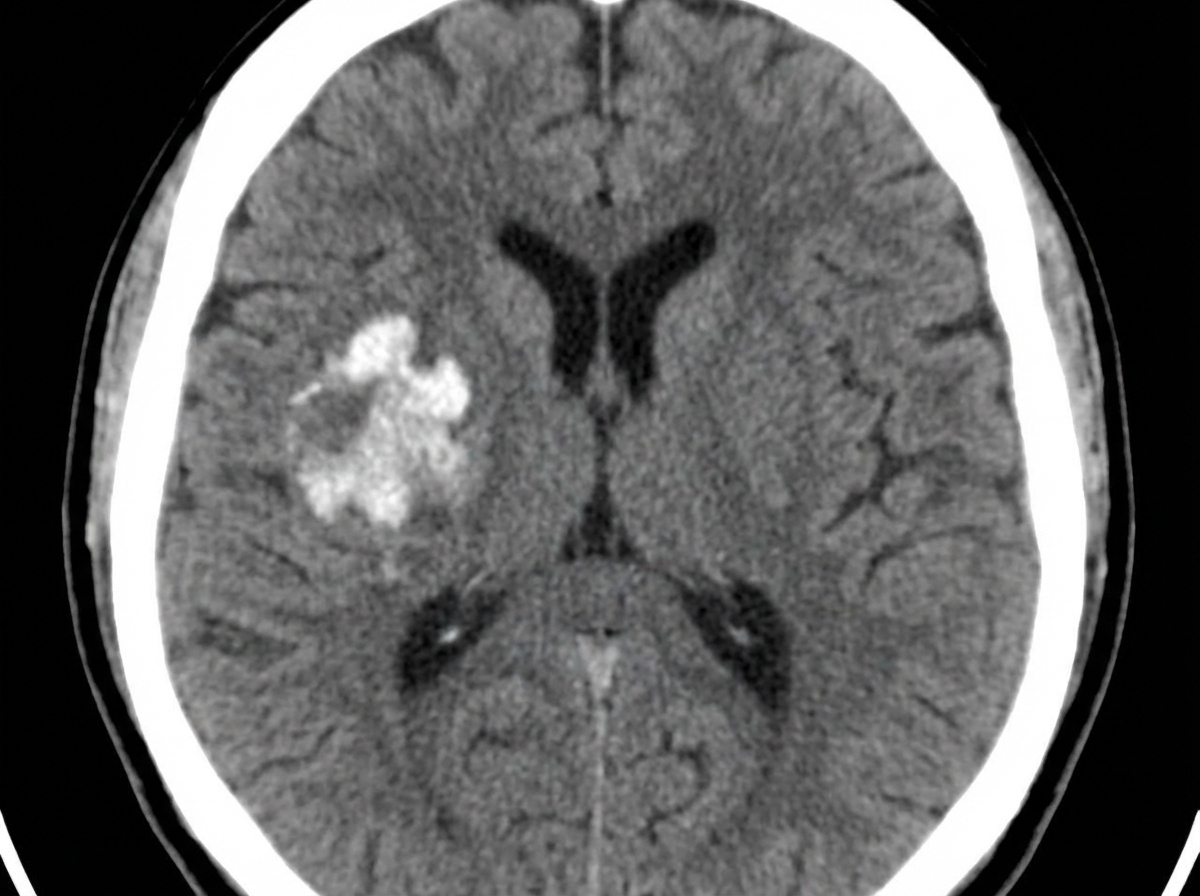
The NCCT shows the presence of which of the following?
In cerebral angiography, in which vessel is the dye injected?
Basal ganglia calcification is seen in all of the following conditions, EXCEPT:
The 'delta sign' on CT is characteristic of which of the following conditions?
Which of the following is not true regarding ossified posterior longitudinal ligament (OPLL)?
The dense middle cerebral artery (MCA) sign is seen in which of the following conditions?
Widened Bat wing sylvian fissures are associated with which of the following conditions?
A child presents with raised ICT; on CT scan, a lesion is seen around the foramen of Monro and multiple periventricular calcific foci are noted. What is the most probable diagnosis?
What is the investigation of choice for the diagnosis of a posterior fossa tumor?
Tear drop sign is seen in:
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app