
Neuroradiology — MCQs

On this page
An elderly patient presented with sudden onset of headache and altered sensorium and is diagnosed to have Subarachnoid hemorrhage. What is the best investigation of choice in this case?
A 20-year-old female presents with a mass in the cavernous sinus and 6th cranial nerve palsy. A T2W MRI shows a hyperintense shadow with homogenous contrast enhancement. What is the most likely diagnosis?
Which of the following conditions is characterized by the 'racing car sign' on imaging?
A 47-year-old female presents with a 2-year history of headache, changes in vision, and seizures. She has recently developed unilateral weakness. A CT scan revealed a well-circumscribed mass abutting the skull in the left hemisphere. Contrast-enhanced MRI confirms the findings. What is the next step in management?
In which of the following conditions is the alanine peak observed on MR Spectroscopy?
What is the most common tumor of the head that undergoes calcification?
A 16-year-old boy complains of headaches for the past 9 months with no prior medical problems. Physical examination reveals no abnormal findings. A CT scan of the head shows enlargement of the lateral cerebral ventricles and third ventricle. Lumbar puncture with normal opening pressure yields clear CSF with slightly elevated protein, normal glucose, and no leukocytes. Which of the following intracranial lesions is most likely to cause these findings?
What is the investigation of choice for laryngeal cartilage involvement?
What is the investigation of choice for an acoustic neuroma measuring 1 cm in diameter?
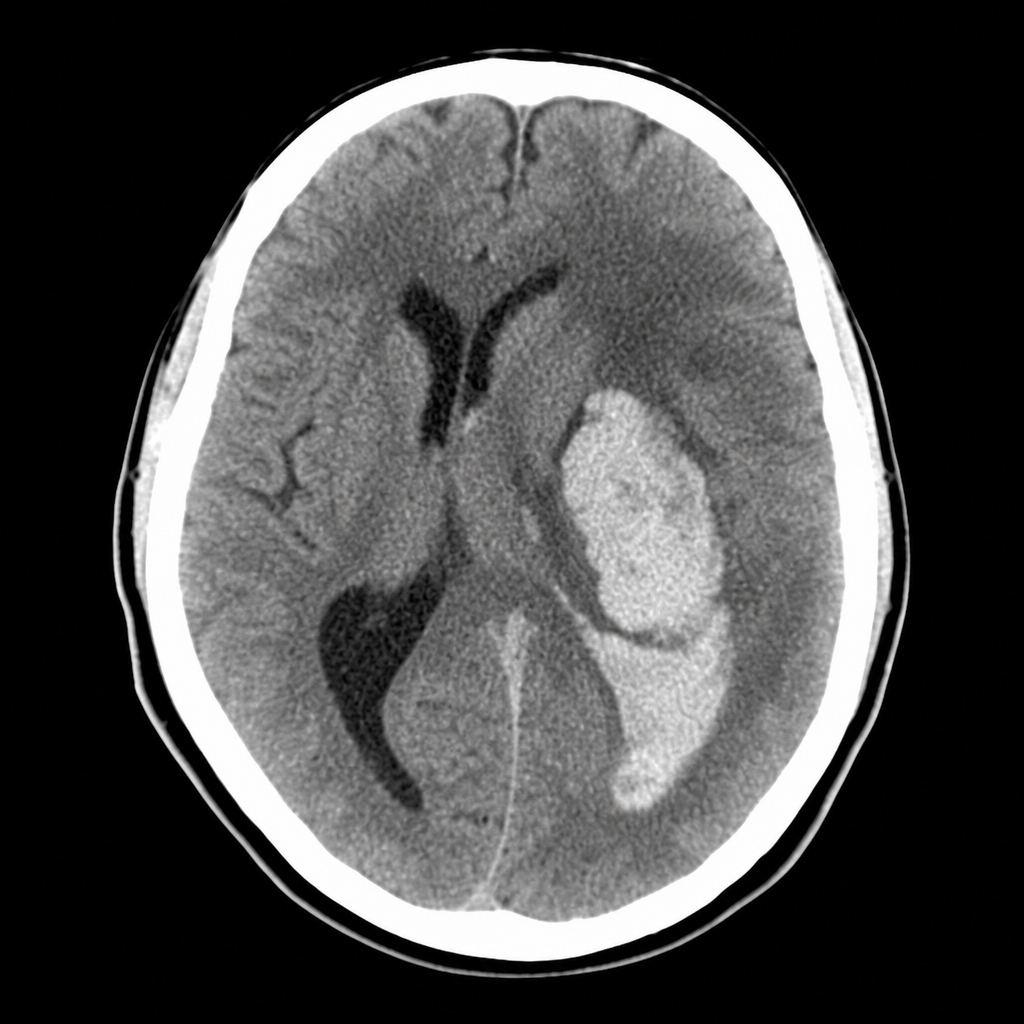
The NCCT shows the primary hemorrhage location to be which of the following?
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app