
Neuroradiology — MCQs

On this page
All are features of raised intracranial tension in adults except?
Which of the following is a cystic supratentorial tumor?
In subarachnoid hemorrhage, where is blood most commonly collected in the skull?
A 28-year-old man presented with headache. A CT head shows a low attenuation mass in the left temporoparietal region which has a similar density to CSF and shows no enhancement following contrast administration. Diffusion-weighted MRI shows high signal. Which of the following is the most probable diagnosis?
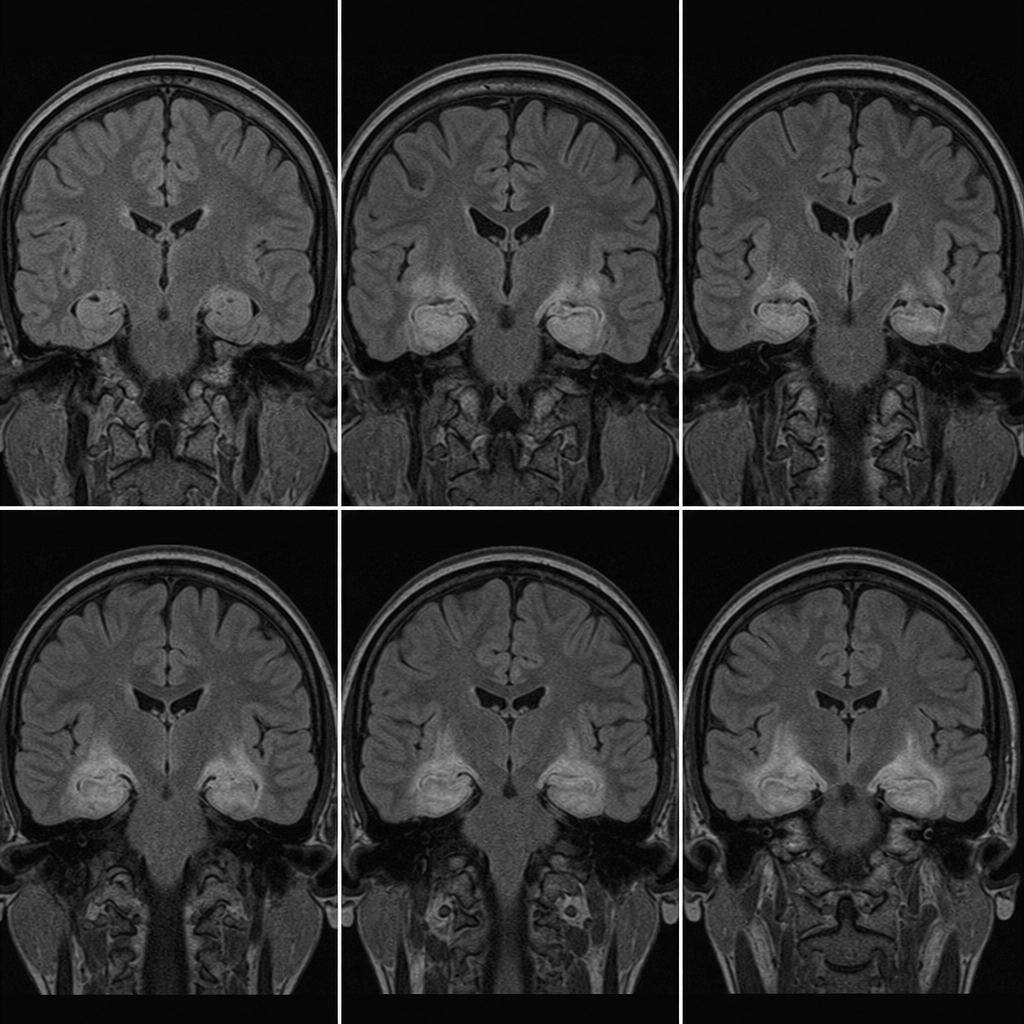
A female patient with breast cancer presents with altered sensorium. What does the following MRI suggest?
In idiopathic basal ganglia calcification, which structure is most often calcified?
Basal ganglia calcification is seen in all of the following conditions except:
What is the investigation of choice for SCIWORA?
Which of the following is NOT a radiological feature of meningioma?
What is true about the MRI/CT appearance of a lateral meningocele?
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app