
Neuroradiology — MCQs

On this page
Intracranial calcification is characteristic of which of the following conditions?
What is the best radiographic view for a fracture of the C1-C2 vertebrae?
J-shaped sella is/are seen in which of the following conditions?
What is the investigation of choice for temporal bone injury?
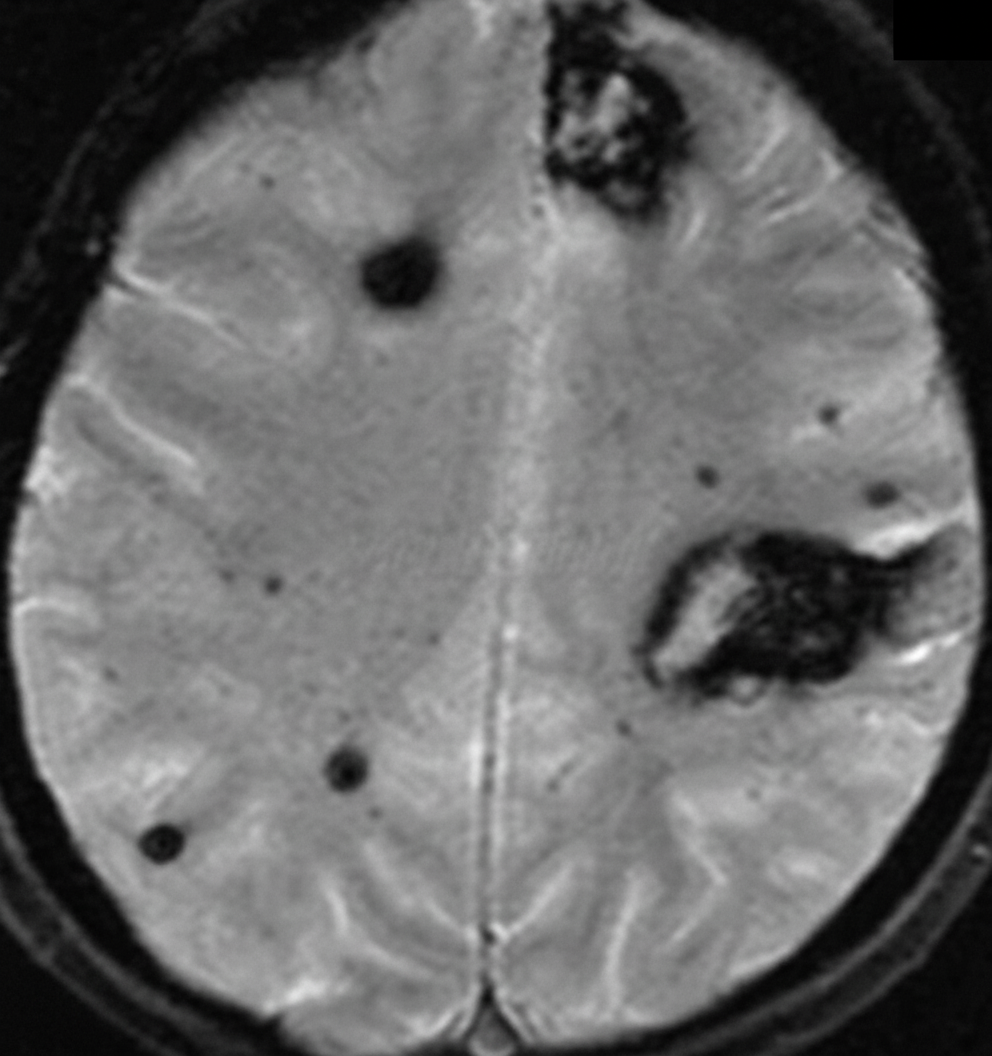
A 40-year-old man presented to the emergency room with loss of consciousness following a high-energy motor vehicle collision. He is a known alcoholic and hypertensive. His non-contrast CT head showed no lesion explaining the coma, and his GCS is 8. An urgent MRI was performed. What is the most likely diagnosis?
Which condition is characterized by 'tram-track calcification' in the brain?
A patient presented with contralateral hemiplegia and sub-periosteal bleeding. What is the initial investigation of choice?
A male was brought unconscious to the hospital with external injuries. CT brain showed no midline shift, but basal cisterns were compressed with multiple small hemorrhages. What is the diagnosis?
A 45-year-old man with AIDS presents with misperceptions, tiredness, and memory loss. Which imaging feature favors a diagnosis of progressive multifocal leukoencephalopathy over HIV encephalopathy?
What condition is associated with the "Radial Band" sign on MRI Brain?
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app