
Neuroradiology — MCQs

On this page
Which one of the following tumors shows calcification on CT Scan?
Presence of calcification on an intracranial lesion is best made out by?
Which CT view is best for evaluating paranasal sinus polyps?
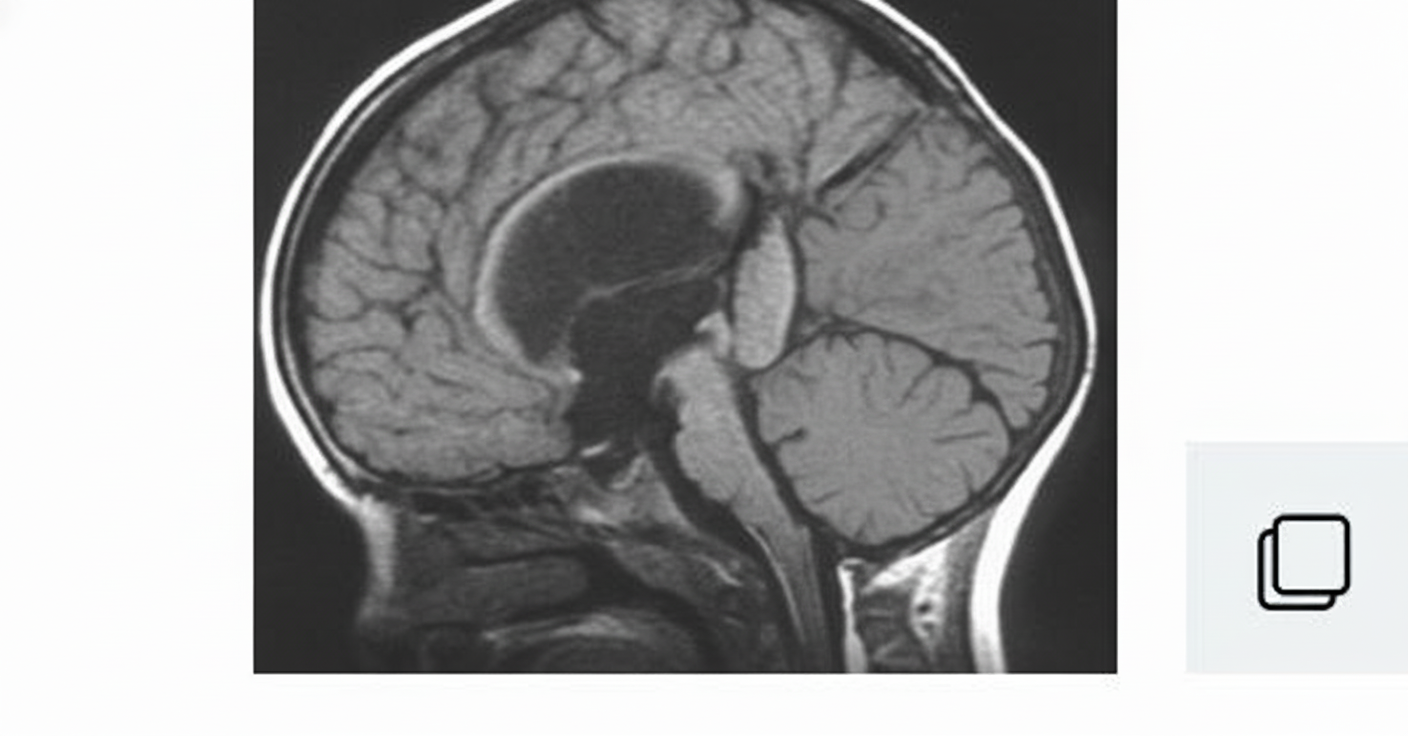
What is your diagnosis in this infant who was found to have hydrocephalus?
Dumb-bell appearance of spinal cord tumours is seen in which of the following?
"Lemon sign" and "Banana sign" on Antenatal Ultrasound are seen in which condition?
What is the first investigation of choice for a spinal cord tumor?
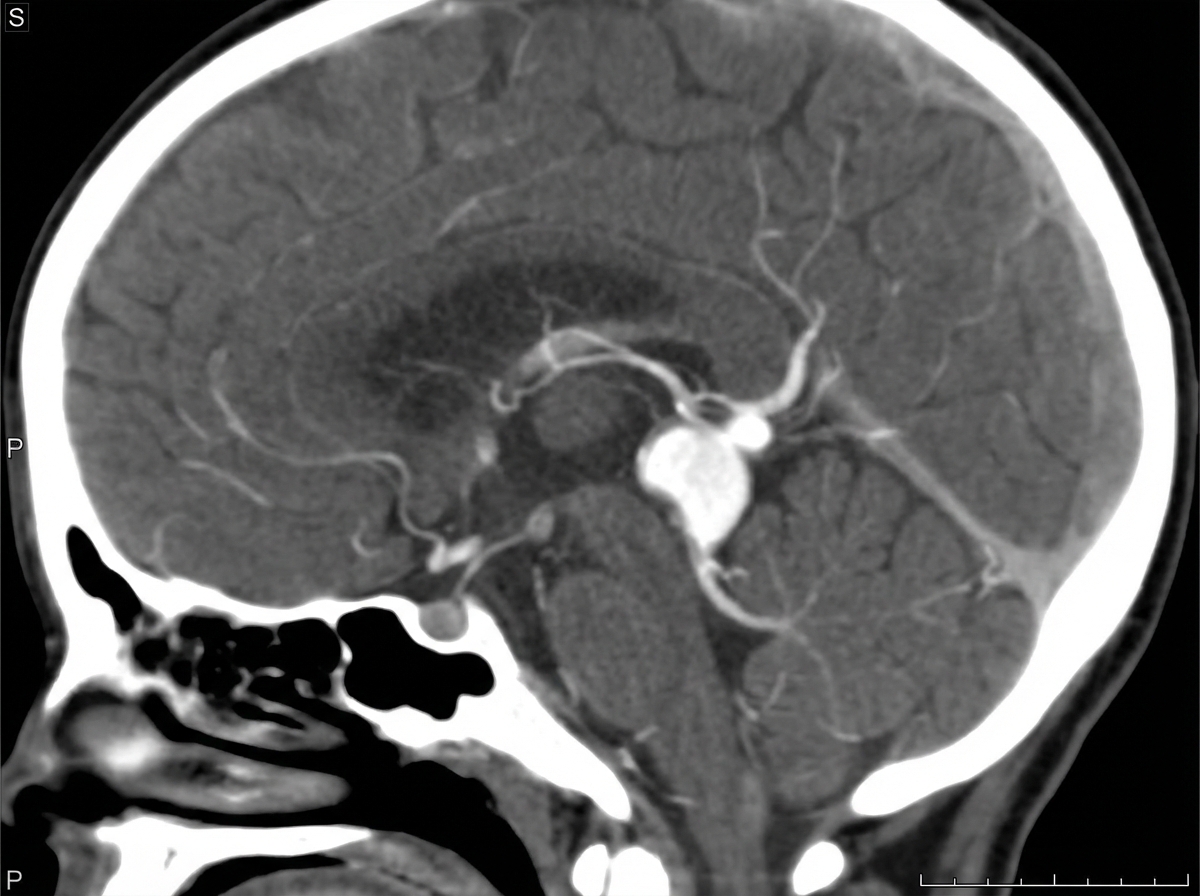
A neonate presents with a high-flow intracranial arteriovenous shunt and high cardiac output heart failure. CT angiography of the neonate is shown. What is the diagnosis?
Calcification of the Posterior Longitudinal Ligament is best diagnosed by which imaging modality?
Which of the following is FALSE regarding Dandy-Walker malformation?
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app