
Neuroradiology — MCQs

On this page
What is the earliest sign of raised intracranial tension on a skull X-ray in infants?
Which condition is characterized by the MRI finding of "tectal beaking"?
The "Eye of the Tiger" appearance in MRI is seen in which of the following conditions?
Which of the following is a characteristic radiological finding of an epidermoid cyst?
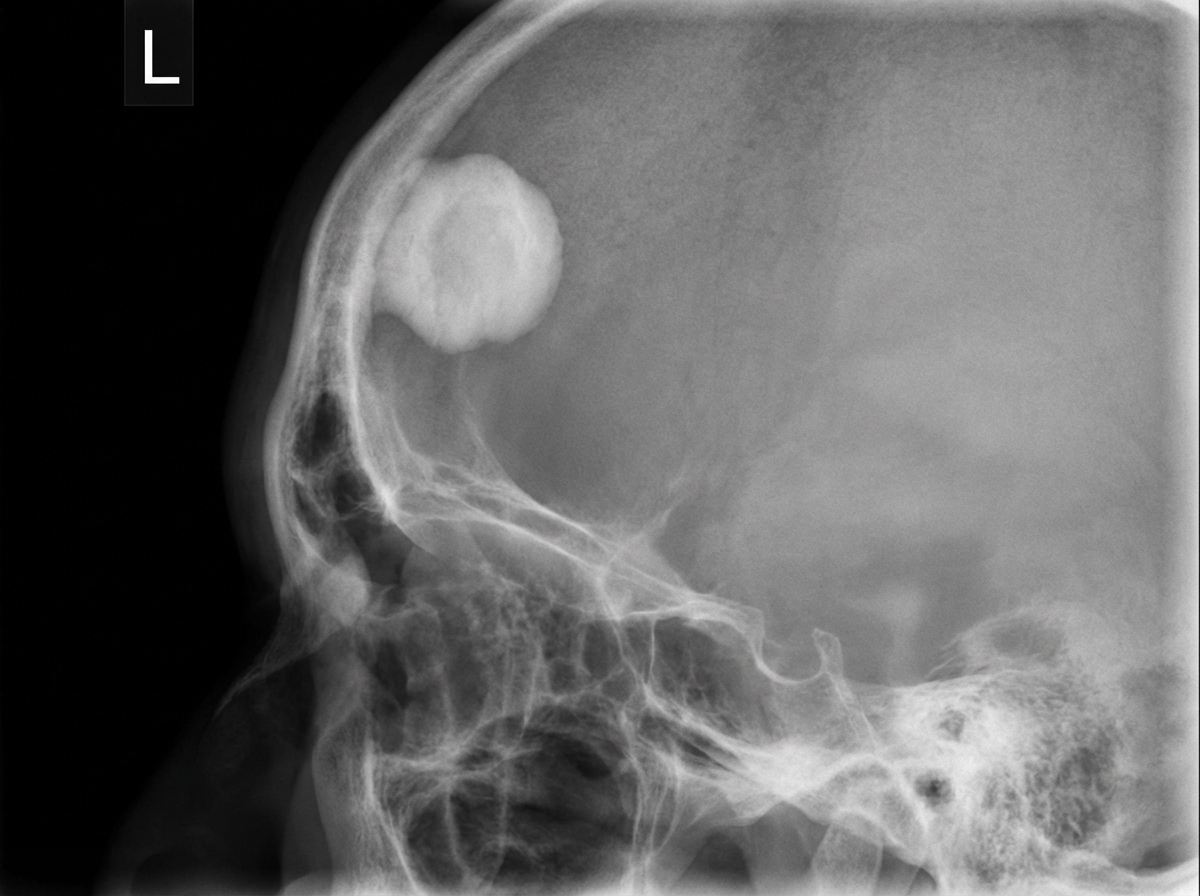
An X-ray film of the skull is provided. What is the diagnosis?
Extensive involvement of deep white matter with hyperdense thalamic lesion on non-contrast CT scan of the brain is seen in which of the following conditions?
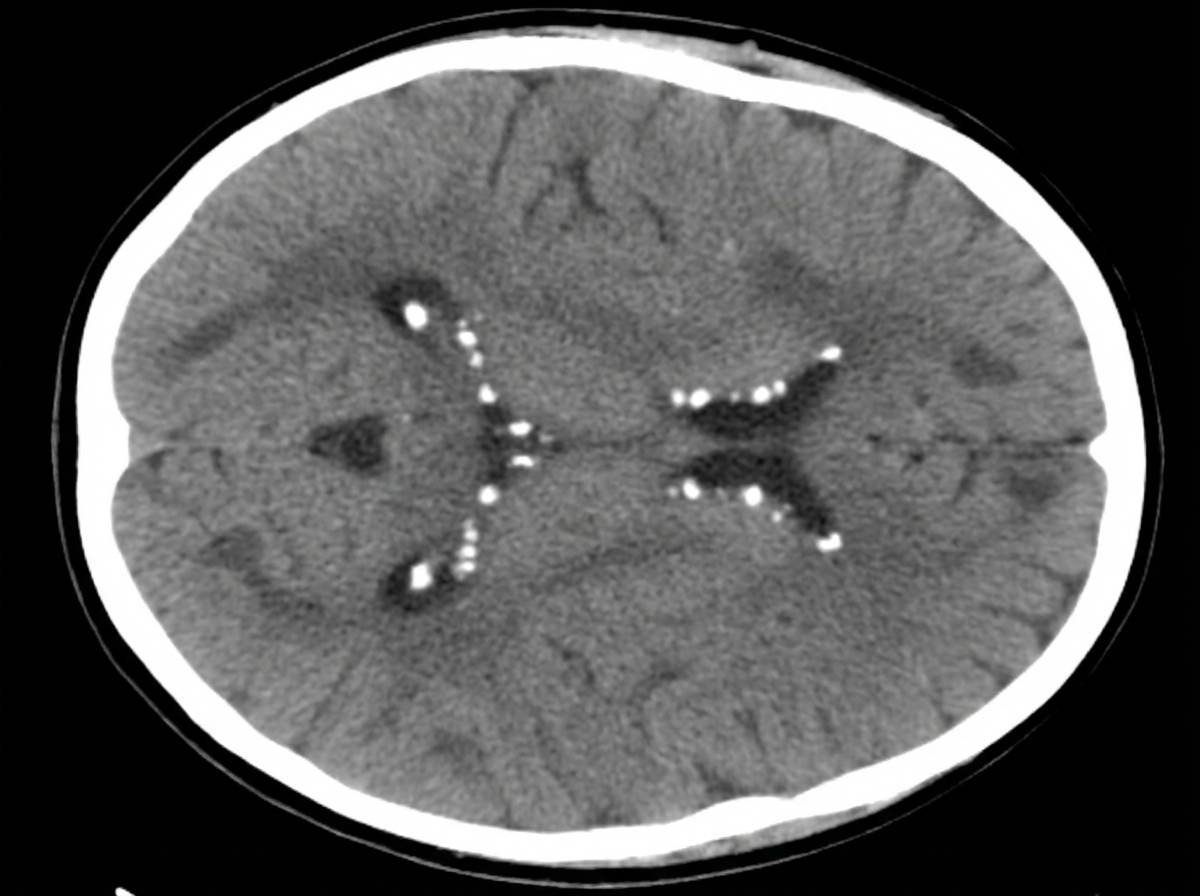
A 12-year-old boy presents with seizures. His mother reports multiple previous hospitalizations for difficult-to-control seizures. A CT scan was performed. What is the diagnosis?
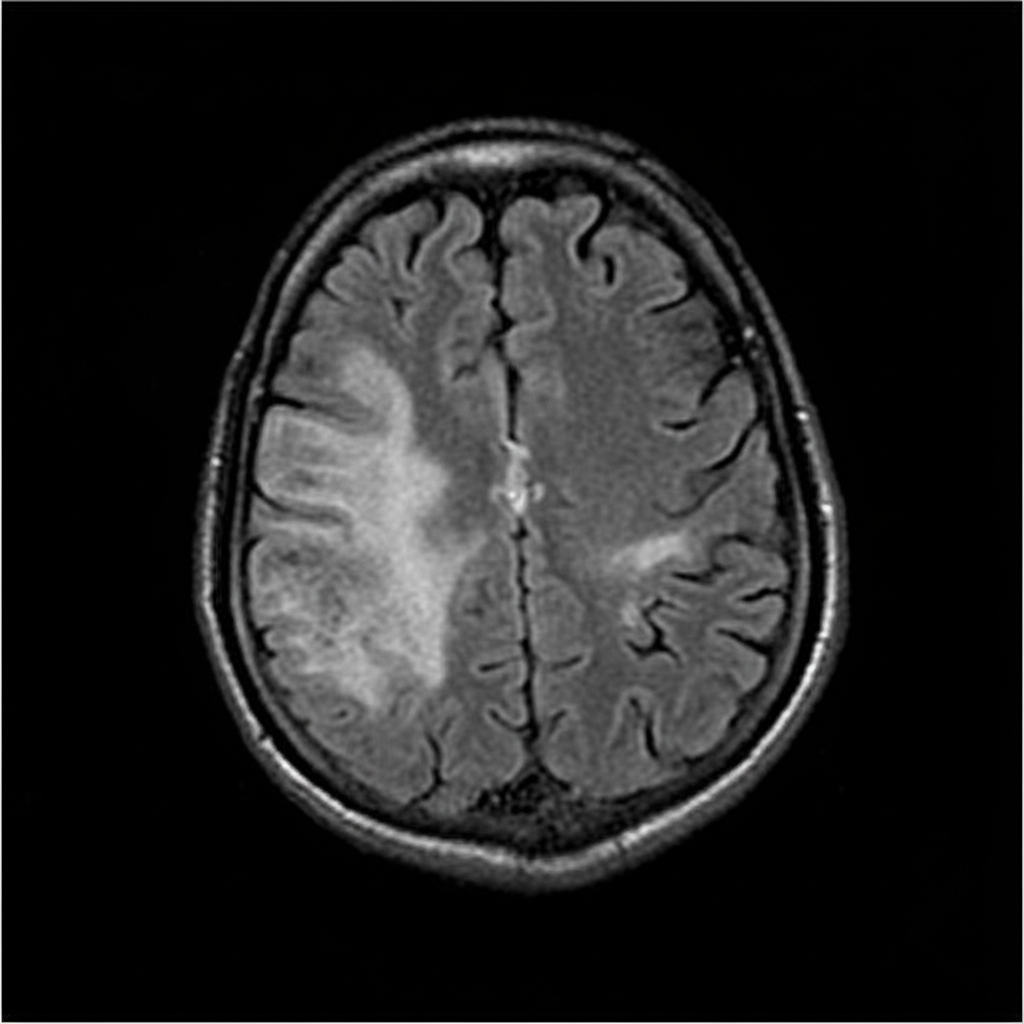
The MRI finding shown in the image is characteristic of which of the following pathologies?
Which of the following imaging sequences is most useful in differentiating between an arachnoid cyst and an epidermoid cyst?
Which one of the following tumors shows calcification on CT Scan?
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app