
Neuroradiology — MCQs

On this page
What is the characteristic 'thumb sign' on CT head indicative of?
Dawson's fingers on MRI are diagnostic of which condition?
Since 15-20 days, a 40-year-old man is unable to look properly upwards. On CT scan study, a cystic lesion within the inferior oblique muscle with probable mural eccentric 'dot' is noted. What is the most-likely diagnosis?
Which of the following is the classic CT appearance of an acute subdural hematoma?
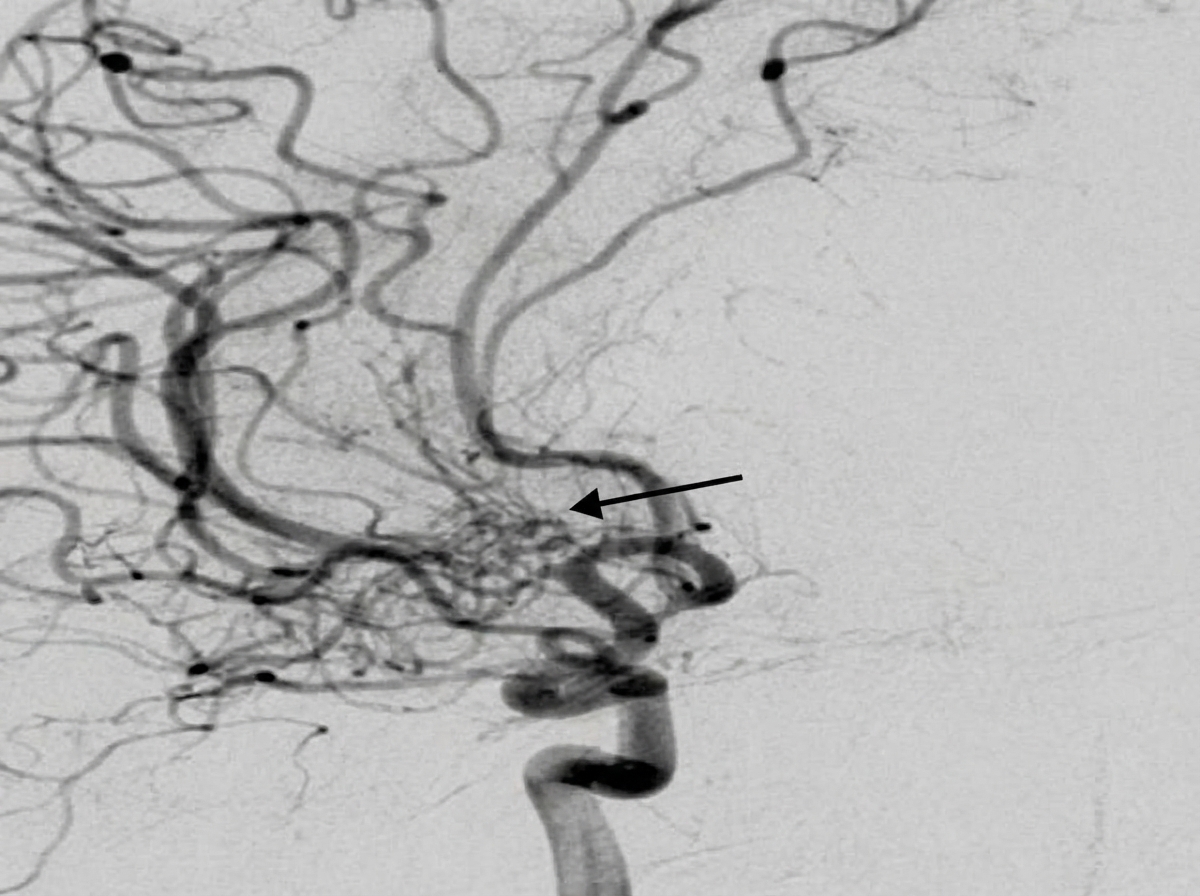
A 20-year-old man presented with epistaxis. DSA showing the sphenopalatine branch of the maxillary artery is provided. The arrow most likely points to which pathology?
The 'swirl sign' is associated with which of the following conditions?
Abnormal signals in bilateral thalami on MRI brain are seen in which of the following conditions?
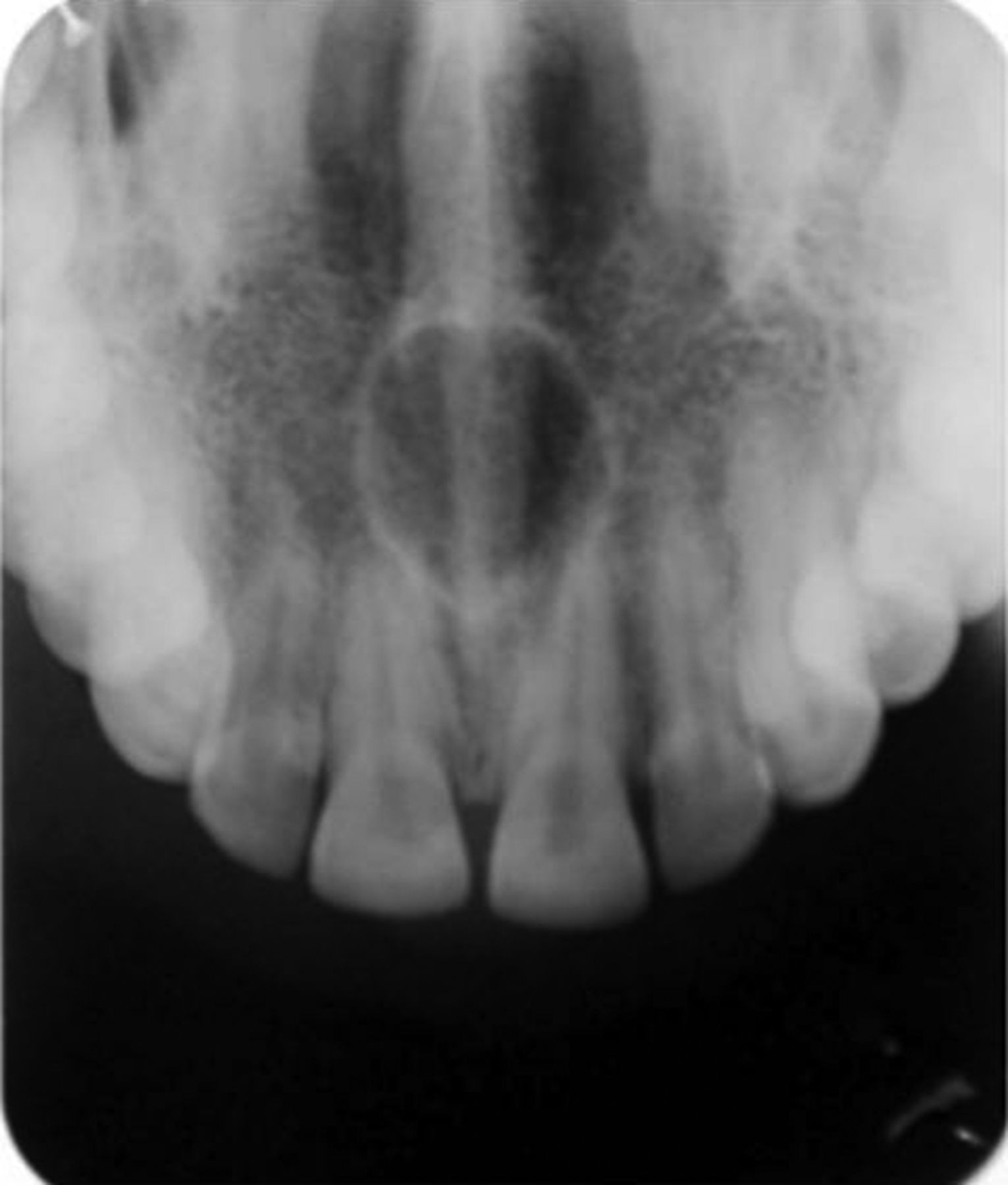
The radiolucency shown by the following radiograph is due to:
A 57-year-old woman, a smoker of 1 pack/day for 40 years, presents with new-onset generalized seizures of approximately 1 minute duration, witnessed by her husband. She has experienced a 25 lb weight loss in the past 3 months. Examination reveals she is thin and nervous, with otherwise normal neurological findings. Chest radiographs show a 4-cm nodule in the right upper lung lobe. To exclude cerebral metastasis as a cause of her seizure, what should be the next diagnostic test?
Which sequence of MRI is used to detect microhemorrhages?
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app