
Neuroradiology — MCQs

On this page
Wine glass appearance on T2W-MRI Brain is seen with which condition?
All of the following are MRI features of Mesial temporal sclerosis, except:
Trouser leg appearance in myelography is typically seen in which type of spinal cord tumor?
Diffuse axonal injury is best detected by which imaging modality?
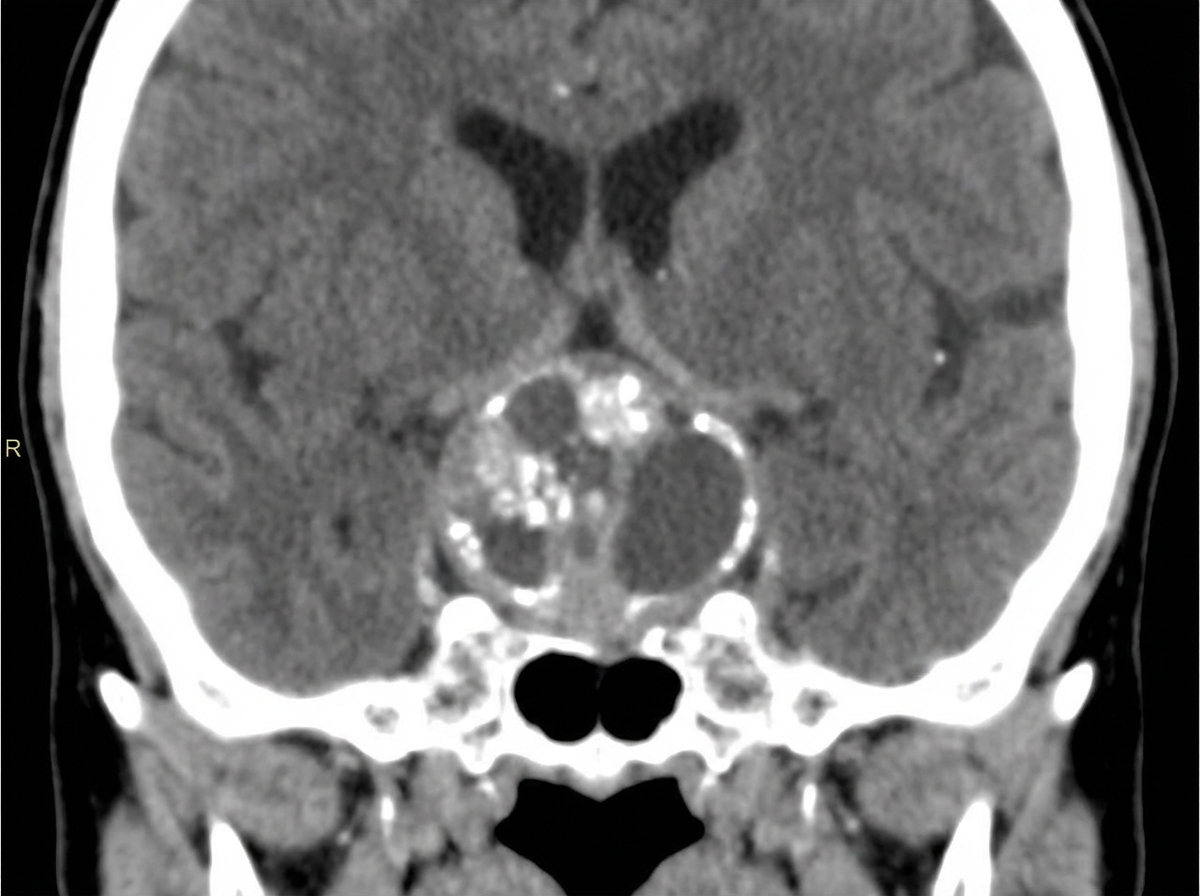
What is the diagnosis for a 10-year-old child presented with vision problems, given the CT scan below?
What is the imaging study of choice for the paranasal sinuses?
What does a angiogram of the basilar artery bifurcation show?
Which of the following is characteristic of Lhermitte-Duclos disease?
Which of the following techniques is best for differentiating recurrence of a brain tumor from radiation therapy-induced necrosis?
A patient presents with proptosis and abducent nerve palsy. A dark homogenous mass is seen on T2W MRI, which shows intense enhancement with contrast. What is the diagnosis?
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app