
Neuroradiology — MCQs

On this page
On MRI, how can epidermoids be differentiated from arachnoid cysts?
A patient presents with loss of consciousness following a road traffic accident. CT scan shows multiple spotty hemorrhages and full basal cisterns. What is the most likely diagnosis?
Which MRI sequence is used to detect cytotoxic edema before vasogenic edema?
Which type of hemorrhage classically presents as a lenticular shape on imaging?
What is the imaging modality of choice for diagnosing brain metastases?
In intervertebral disc prolapse, what does a Schmorl node on MRI imply?
Focal bilateral thalamic, posterior internal capsule showing hyperdensity and calcification in CT scan and extensive involvement of deep white matter is characteristic of which condition?
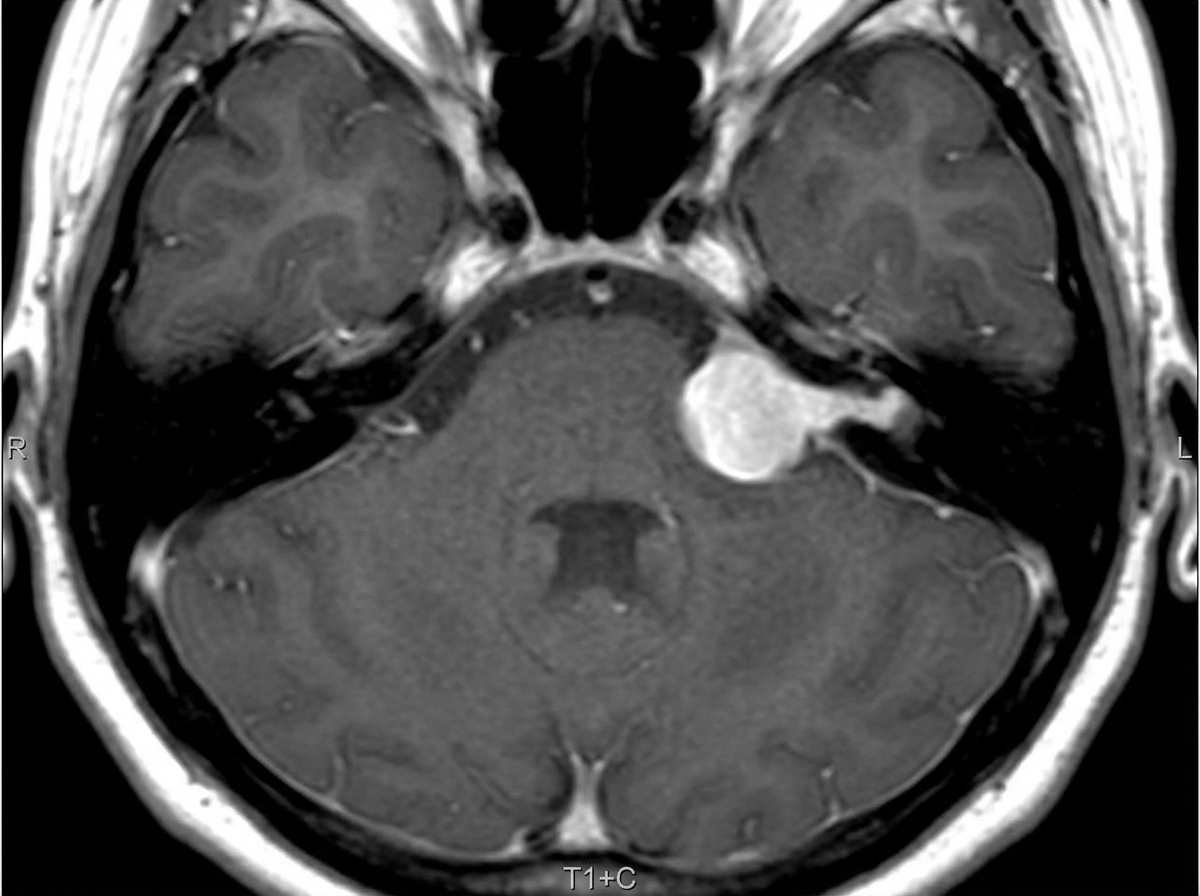
This classical "Ice-cream cone" appearance of an intensely enhancing lesion at the left CP angle recess suggests:
A tumour showing dural enhancement with a tail is characteristic of which of the following entities?
What condition is characterized by a "tram track" appearance on a CT scan of the head?
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app