
Neuroradiology — MCQs

On this page
Bony clival erosion with intracranial calcification is seen in which of the following?
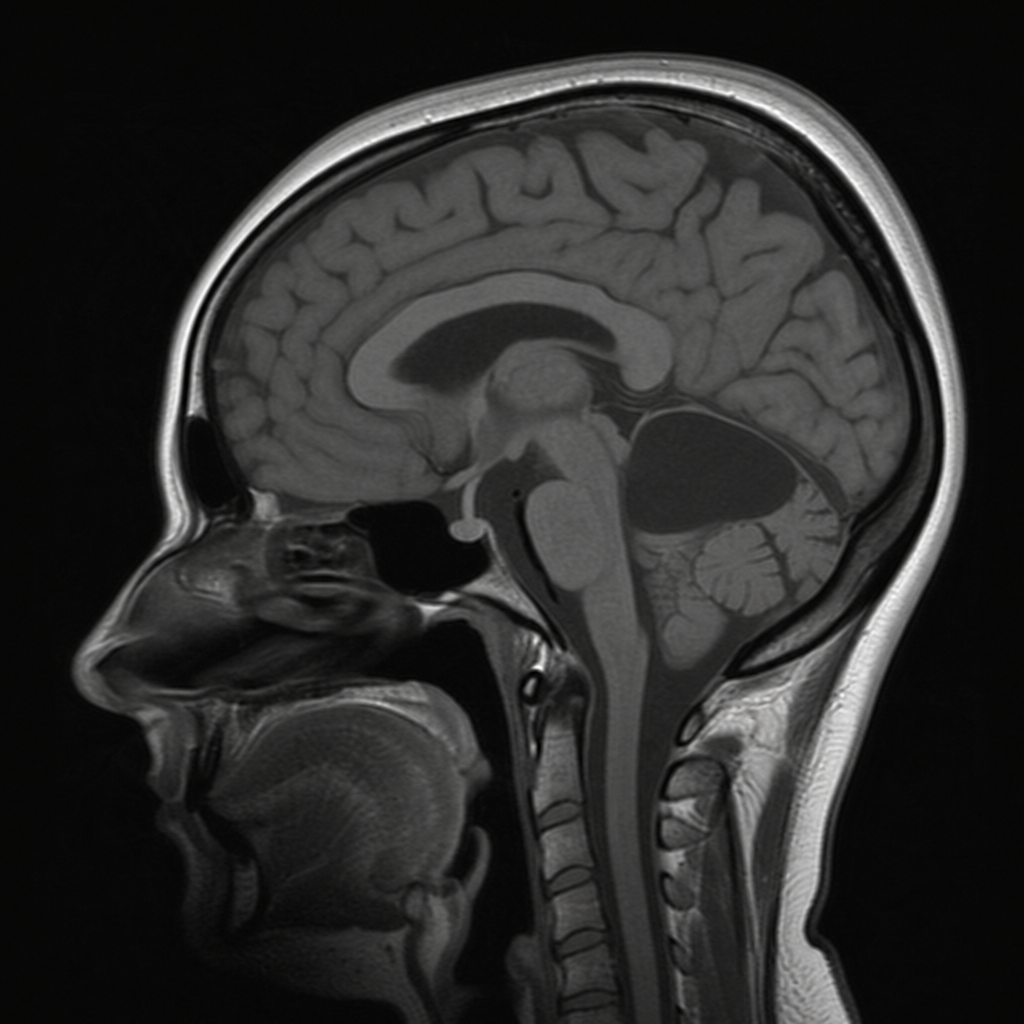
Which of the following is represented by an MRI of the skull?
Which leukodystrophy characteristically presents with bilateral occipital lobe involvement?
What is the imaging modality of choice in the setting of head trauma?
Which area of the thalamus is involved in Wernicke's encephalopathy?
A 45-year-old female presents with headache, vomiting, and deterioration of consciousness, two years after resection of a parietal lobe brain tumor. What is the most appropriate investigation to perform now?
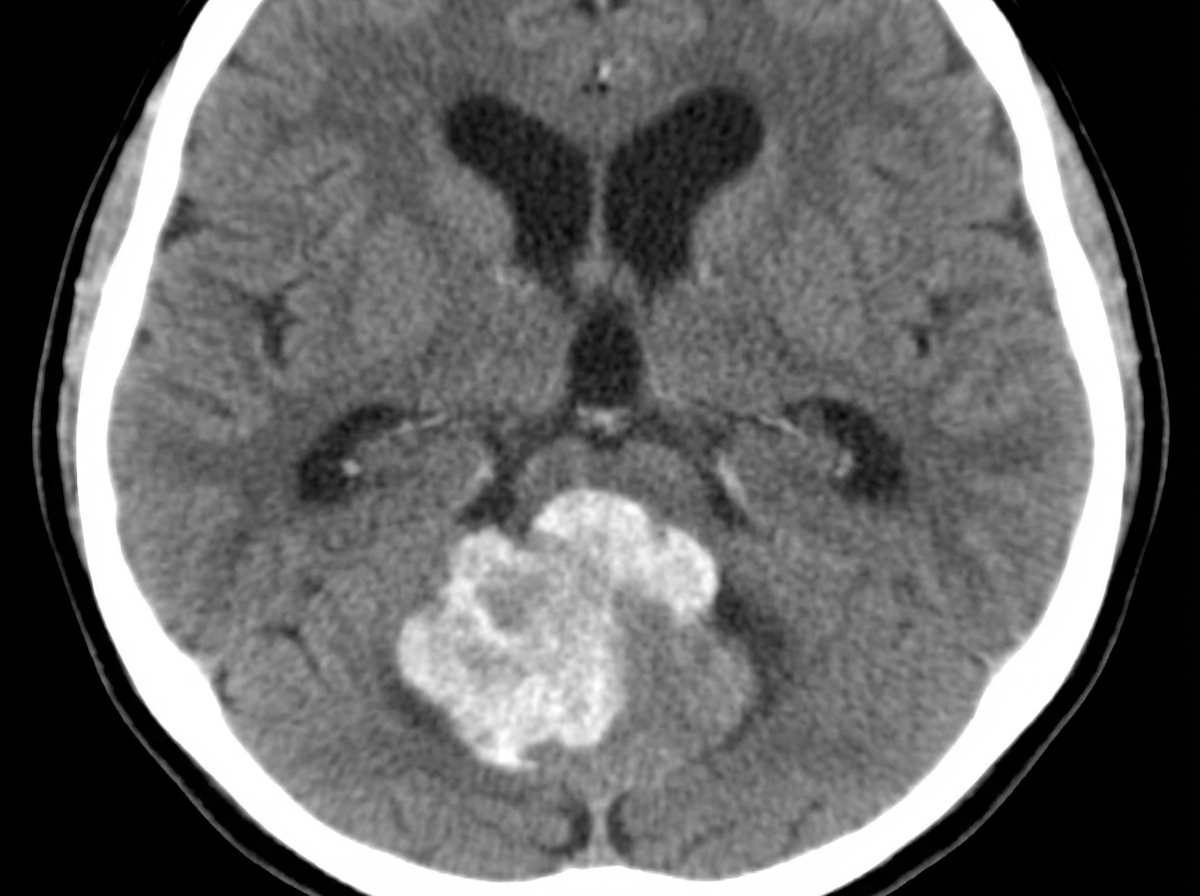
The given CT scan shows which brain lesion?
The provided MRI of the spine denotes which of the following findings?

What is the most definitive test for evaluating intracranial aneurysms?
J-Shaped sella turica is seen in which condition?
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app