
Neuroradiology — MCQs

On this page
A 12-year-old boy is rushed to the emergency room in a coma after falling from an upper story window of his home. MRI shows a subdural hematoma over the left hemisphere. What is the most likely source of intracranial bleeding in this patient?
Which of the following findings would distinguish hydrocephalus due to aqueductal stenosis from hydrocephalus due to Dandy-Walker malformation?
Meningioma on plain radiography reveals which of the following findings?
What is the best radiographic view for visualizing the mandible?
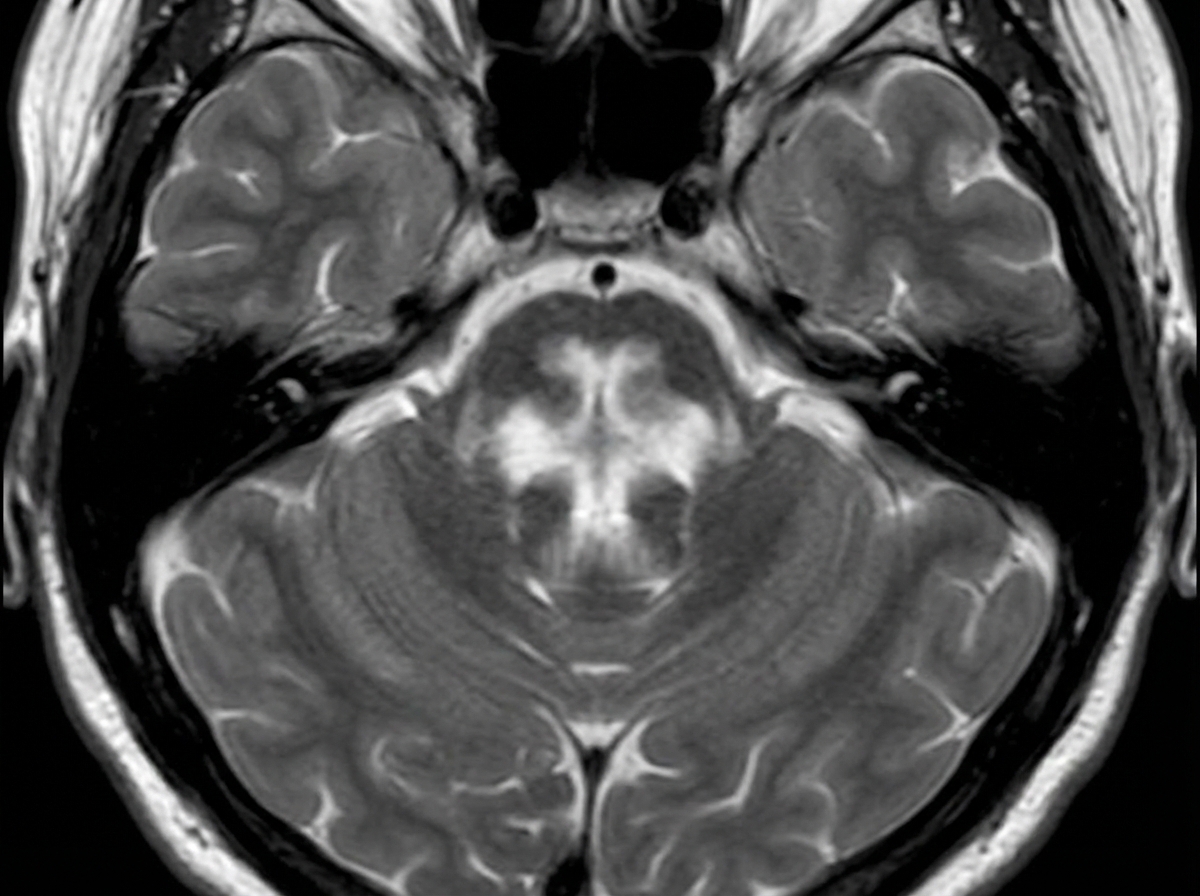
The 'Hot Cross Bun' sign on MRI is characteristically seen in which of the following conditions?
Premature filling of veins is a manifestation in cerebral angiography of which condition?
A 37-year-old man with AIDS presents with confusion, lethargy, and memory loss. CT of the brain demonstrates multiple supratentorial enhancing masses. Which imaging feature favors a diagnosis of toxoplasmosis rather than primary CNS lymphoma?
What condition is characterized by a "puff of smoke" appearance on contrast CT angiography?
A 60-year-old male patient presented with spasticity in bilateral lower limbs, gait ataxia, dysarthria, and orthostatic hypotension. An MRI was performed and is shown below. What is the most likely diagnosis?
Bony clival erosion with intracranial calcification is seen in which of the following?
Practice by Chapter
Neuroanatomy for Radiologists
Practice Questions
Cerebrovascular Diseases
Practice Questions
Intracranial Tumors
Practice Questions
CNS Infections
Practice Questions
Demyelinating and Degenerative Diseases
Practice Questions
Head Trauma Imaging
Practice Questions
Spine Imaging: Trauma and Degenerative Disease
Practice Questions
Spine Tumors and Infections
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital CNS Anomalies
Practice Questions
Functional Neuroimaging
Practice Questions
Neurointerventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app