
Demyelinating and Degenerative Diseases — MCQs

Which of the following symptoms is least likely to be associated with multiple sclerosis?
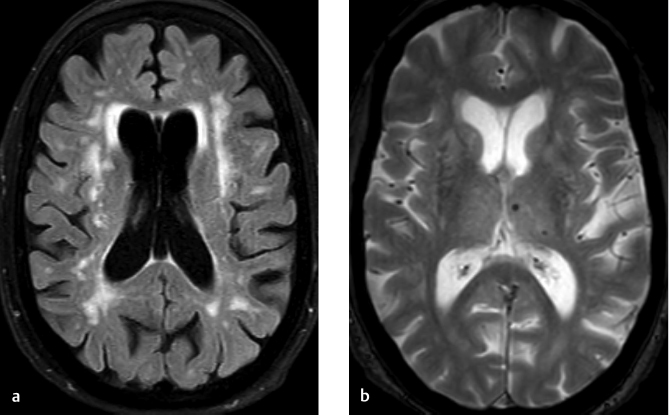
What is the typical MRI finding in multiple sclerosis (MS)?
A 67-year-old male presents with progressive difficulty in walking, frequent falls, and stiffness in the legs. Neurological examination reveals increased muscle tone, brisk deep tendon reflexes, and a positive Babinski sign. MRI of the brain shows multiple white matter lesions. Which of the following is the most likely diagnosis?
Spine MRI shows 'pencil-sharpened' vertebral bodies and 'H-shaped' vertebrae on T1-weighted images. Most likely diagnosis?
Tigroid pattern on MRI is seen in -
A 58-year-old presents with progressive cognitive decline. MRI brain is unremarkable. FDG-PET shows bilateral temporoparietal and posterior cingulate hypometabolism with relative sparing of sensorimotor cortex. Analyze these findings to determine the most likely diagnosis.
How does diffusion-weighted imaging (DWI) detect acute stroke earlier than conventional MRI sequences?
Which imaging modality is best for evaluating retinoblastoma?
Intra-tumoral calcification in the brain is seen in all except?
Which of the following brain tumors is typically hyperdense on CT scan?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app