
Musculoskeletal Radiology — MCQs

On this page
A person has an injury to the forefinger with glass and it is suspected that there is a retained piece of glass in the finger. What is the first investigation you will perform?
A 15-year-old female has an impacted tooth 23, located apical to teeth 22 and 24. How would an oral surgeon determine if the impacted tooth is positioned buccally or palatally to teeth 22 and 24?
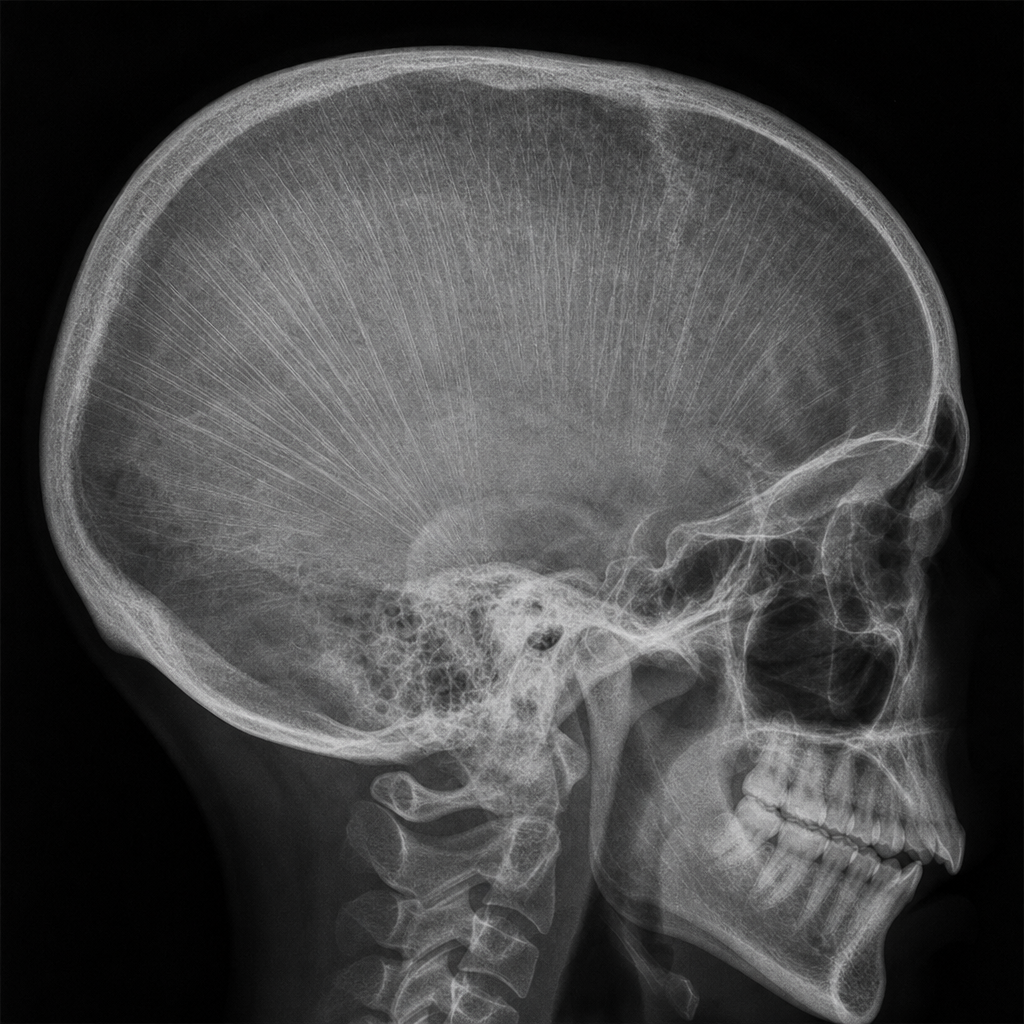
Lines shown in the above skull radiograph are a characteristic feature of which of the following conditions?
A radiograph of a girl's mandible shows a soap bubble appearance of a lytic lesion. On aspiration, the lesion yields blood. A whirring sound is heard from the lesion, and the girl can feel her heartbeat within it. What is the next recommended investigation?
Which condition is characterized by the presence of ring-shaped epiphyses?
A dense metaphyseal band is seen in which condition?
"Bone within bone" appearance is classically seen in?
A young child presents with backache. Imaging reveals a solitary collapsed dorsal vertebra with preserved intervertebral disc spaces and no evidence of a soft tissue mass. What is the most likely diagnosis?
Subcutaneous calcifications are seen in which of the following conditions?
Which imaging view best demonstrates inflammation and temporomandibular joint effusion?
Practice by Chapter
Radiographic Anatomy of Bones and Joints
Practice Questions
Imaging of Fractures and Dislocations
Practice Questions
Arthritides: Inflammatory and Degenerative
Practice Questions
Metabolic Bone Diseases
Practice Questions
Bone and Soft Tissue Tumors
Practice Questions
Congenital Skeletal Anomalies
Practice Questions
Spine Imaging
Practice Questions
Skeletal Infections
Practice Questions
Sports Medicine Imaging
Practice Questions
Imaging of Prostheses and Implants
Practice Questions
Musculoskeletal Ultrasound
Practice Questions
MSK Interventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app