
Musculoskeletal Radiology — MCQs

On this page
Which of the following is NOT a radiological feature of scurvy?
Which of the following investigations is NOT useful in Multiple Myeloma?
Which of the following is not a radiological feature of rickets?
The "tongue-in-groove" or "tottering fence post" appearance of the femur is seen in which of the following conditions?
In lead poisoning, where is lead deposition typically seen on a radiograph?
Looser's zone occurs in which of the following anatomical locations?
Sacrotuberous ligament calcification is a characteristic feature of?
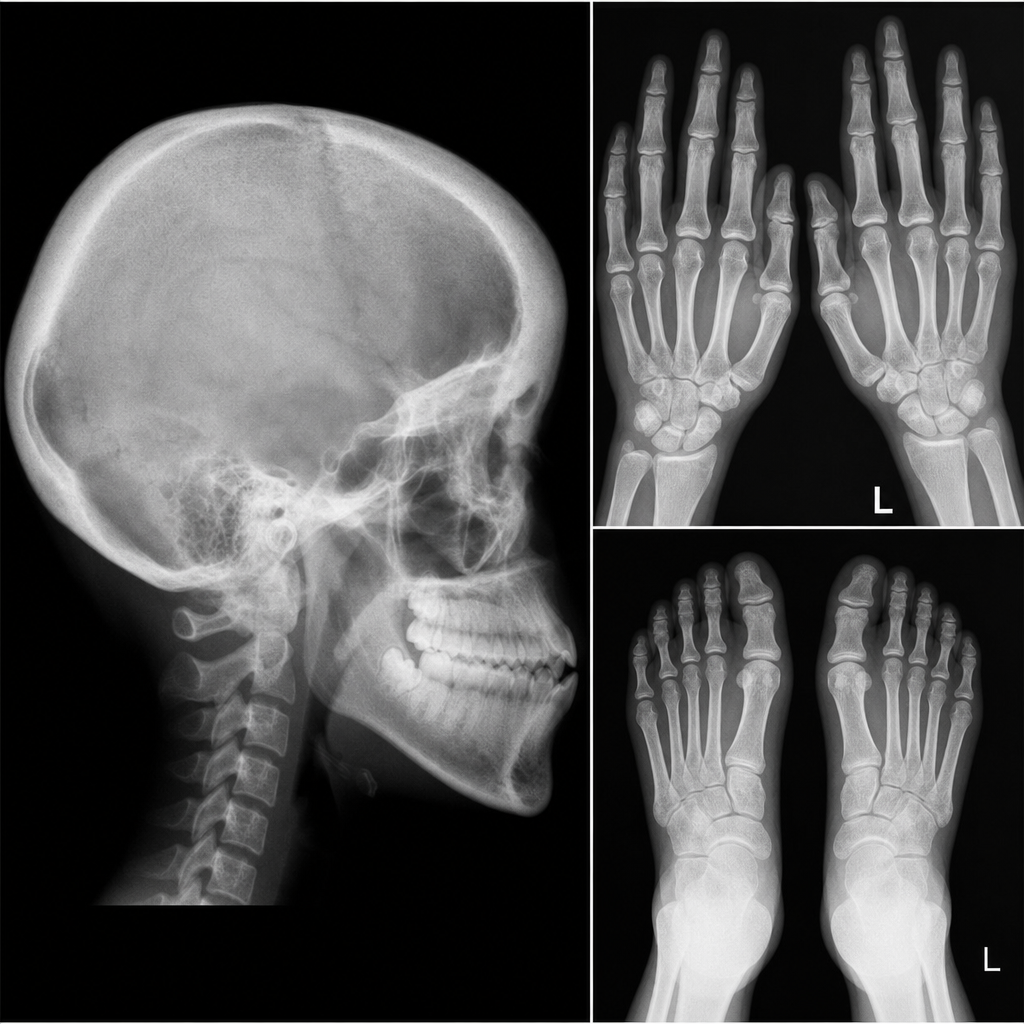
What is the likely diagnosis given this radiological appearance?
Which condition is not characteristically associated with an impacted mandibular third molar?
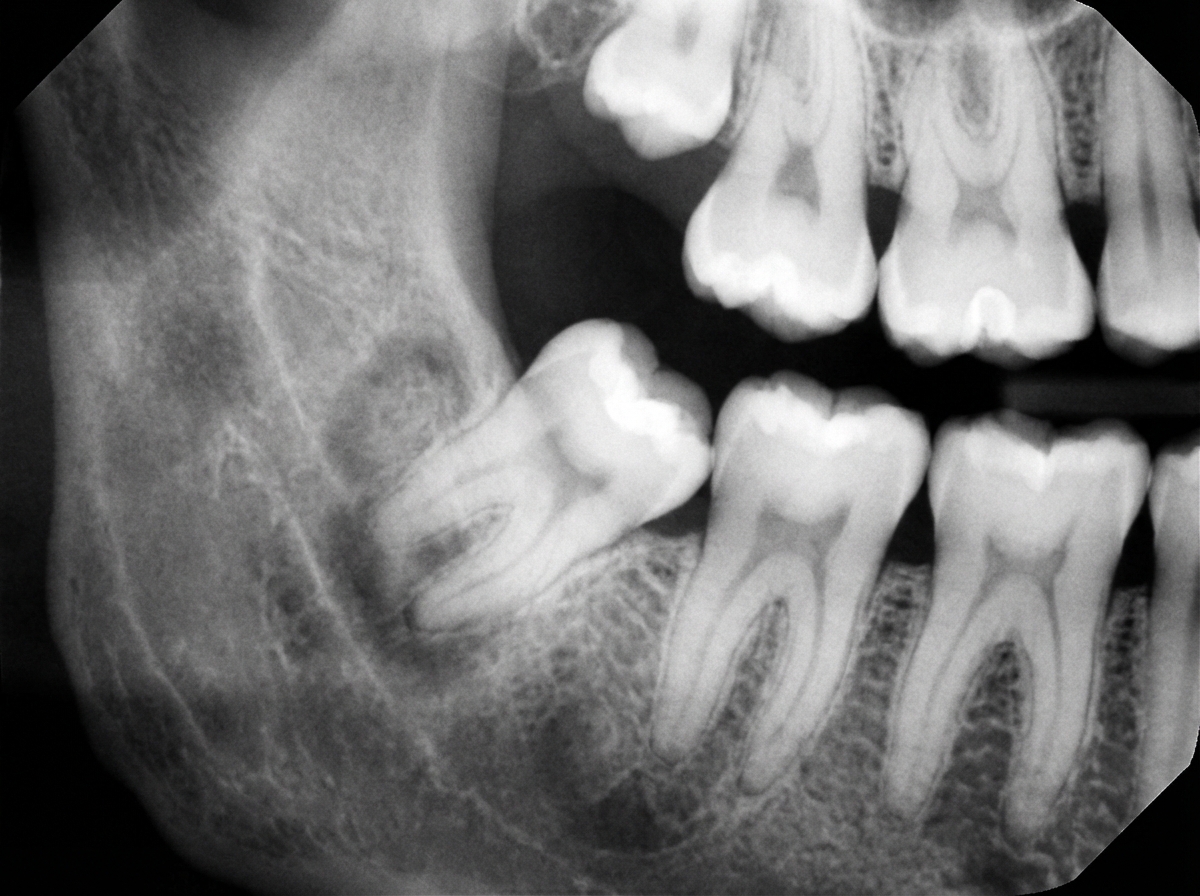
A 60-year-old male reports for denture adjustment. His OPG shows a 1 cm lytic area in the lower bicuspid region. What is the most probable diagnosis?
Practice by Chapter
Radiographic Anatomy of Bones and Joints
Practice Questions
Imaging of Fractures and Dislocations
Practice Questions
Arthritides: Inflammatory and Degenerative
Practice Questions
Metabolic Bone Diseases
Practice Questions
Bone and Soft Tissue Tumors
Practice Questions
Congenital Skeletal Anomalies
Practice Questions
Spine Imaging
Practice Questions
Skeletal Infections
Practice Questions
Sports Medicine Imaging
Practice Questions
Imaging of Prostheses and Implants
Practice Questions
Musculoskeletal Ultrasound
Practice Questions
MSK Interventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app