
Musculoskeletal Radiology — MCQs

On this page
Sunray appearance and Codman's triangle are radiological features of which of the following tumors?
What are the common causes of vertebra plana?
X-ray changes in acromegaly include all of the following except:
The "Shiny Corner Sign" is typically seen in which of the following conditions?
Wimberger's ring is seen in:
Posterior scalloping of vertebrae is seen in all of the following conditions except?
An expansile lytic lesion of the sacrum with specks of calcification is suggestive of which of the following?
Fluid levels are seen in which of the following conditions?
What condition is characterized by this type of lesion?
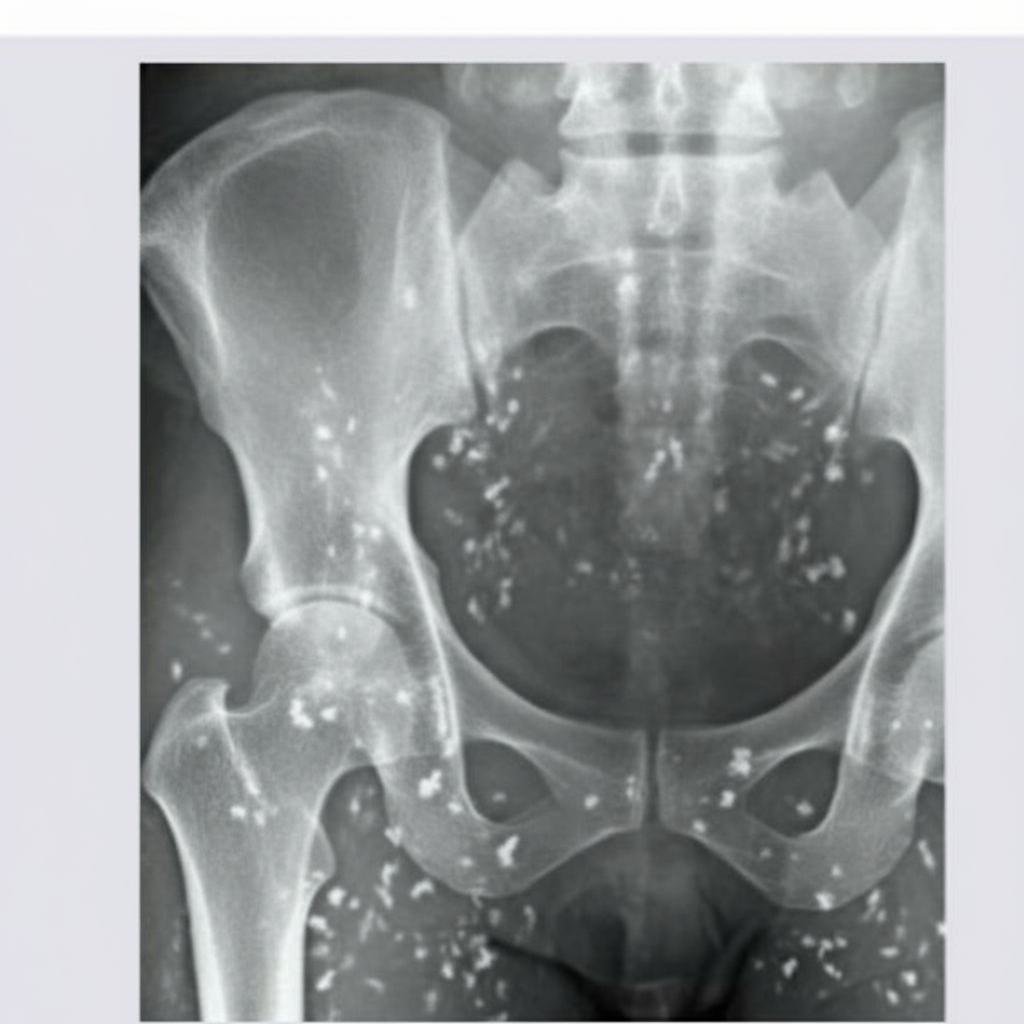
Multiple raindrop osteolytic lesions are seen in which of the following conditions?
Practice by Chapter
Radiographic Anatomy of Bones and Joints
Practice Questions
Imaging of Fractures and Dislocations
Practice Questions
Arthritides: Inflammatory and Degenerative
Practice Questions
Metabolic Bone Diseases
Practice Questions
Bone and Soft Tissue Tumors
Practice Questions
Congenital Skeletal Anomalies
Practice Questions
Spine Imaging
Practice Questions
Skeletal Infections
Practice Questions
Sports Medicine Imaging
Practice Questions
Imaging of Prostheses and Implants
Practice Questions
Musculoskeletal Ultrasound
Practice Questions
MSK Interventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app