
Musculoskeletal Radiology — MCQs

On this page
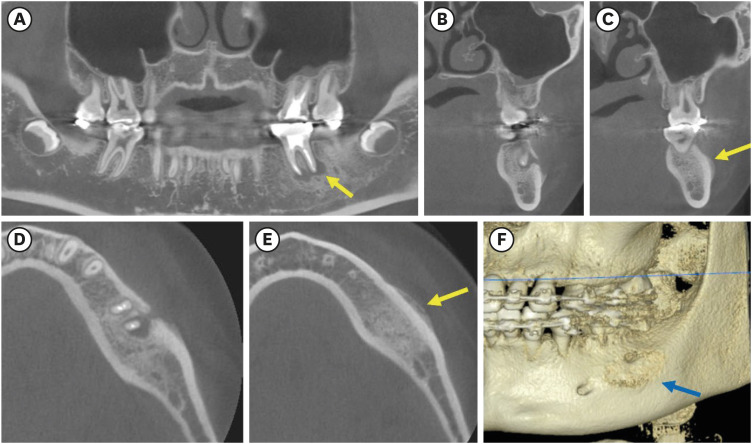
A 12-year-old patient presents with a painless, slowly enlarging swelling of the left posterior mandible for the past 6 months. Clinical examination reveals a firm, non-tender expansion of the mandible, and the adjacent mandibular left second molar is carious with a periapical abscess. Radiographically, the lesion shown in the image could be:
What is the investigation of choice for diagnosing a stress fracture?
X-ray features of hypoparathyroidism are the following except:
All of the following have the same radiographic features except:
The 'Search lines' to detect fracture line on occipitomandibular radiographic view of midfacial skeleton fracture was described by:
"Hair on End" appearance is seen in:
Not a radiological feature of Ankylosing spondylitis
Wimberger sign is seen in ?
Sunburst appearance found in:
Radiological findings of scurvy are A/E:
Practice by Chapter
Radiographic Anatomy of Bones and Joints
Practice Questions
Imaging of Fractures and Dislocations
Practice Questions
Arthritides: Inflammatory and Degenerative
Practice Questions
Metabolic Bone Diseases
Practice Questions
Bone and Soft Tissue Tumors
Practice Questions
Congenital Skeletal Anomalies
Practice Questions
Spine Imaging
Practice Questions
Skeletal Infections
Practice Questions
Sports Medicine Imaging
Practice Questions
Imaging of Prostheses and Implants
Practice Questions
Musculoskeletal Ultrasound
Practice Questions
MSK Interventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app