
Musculoskeletal Radiology — MCQs

On this page
The following X-ray of the pelvis shows:

The given X-ray of the humerus shows:

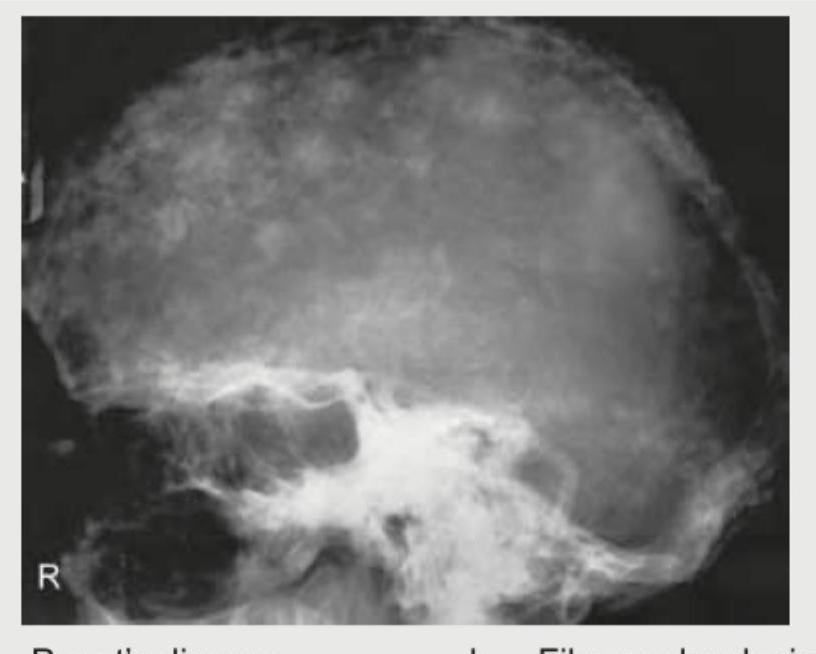
A 65-year-old man presents with bone pains. X-ray Skull shows? (Recent NEET Pattem 2018-19)
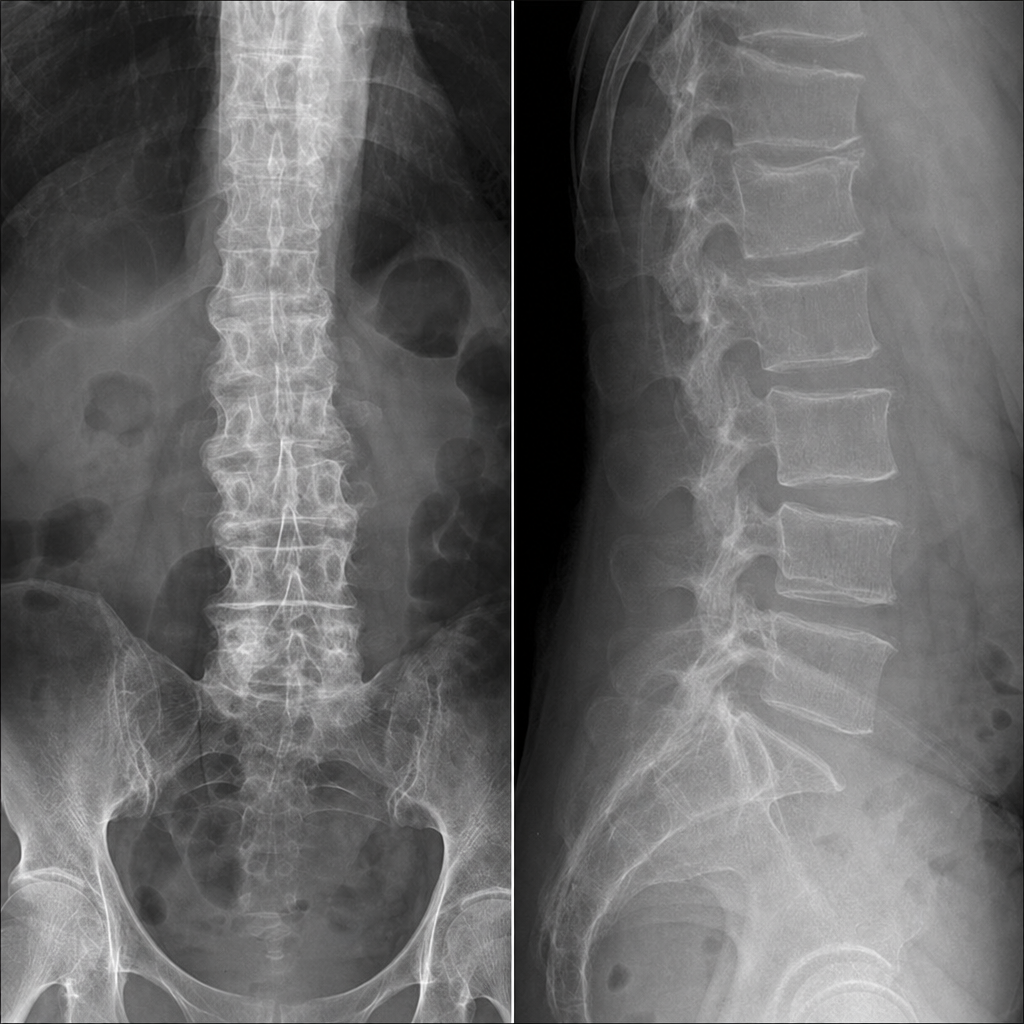
A 75-year-old female has chronic backache. X-ray spine is shown. What is the most likely diagnosis?
A 6-year-old boy presents with severe anemia and organomegaly. Peripheral smear was performed. The X-ray of hand shows:

A middle-aged man presents with a lower jaw swelling. Clinically, there is expansion of the left ramus and the X-ray mandible shows soap bubble appearance. What is the clinical diagnosis?
A man presents with back pain following a road traffic accident (RTA). There is no history of neurological deficit. An X-ray of the spine is done. What is the diagnosis based on the image?

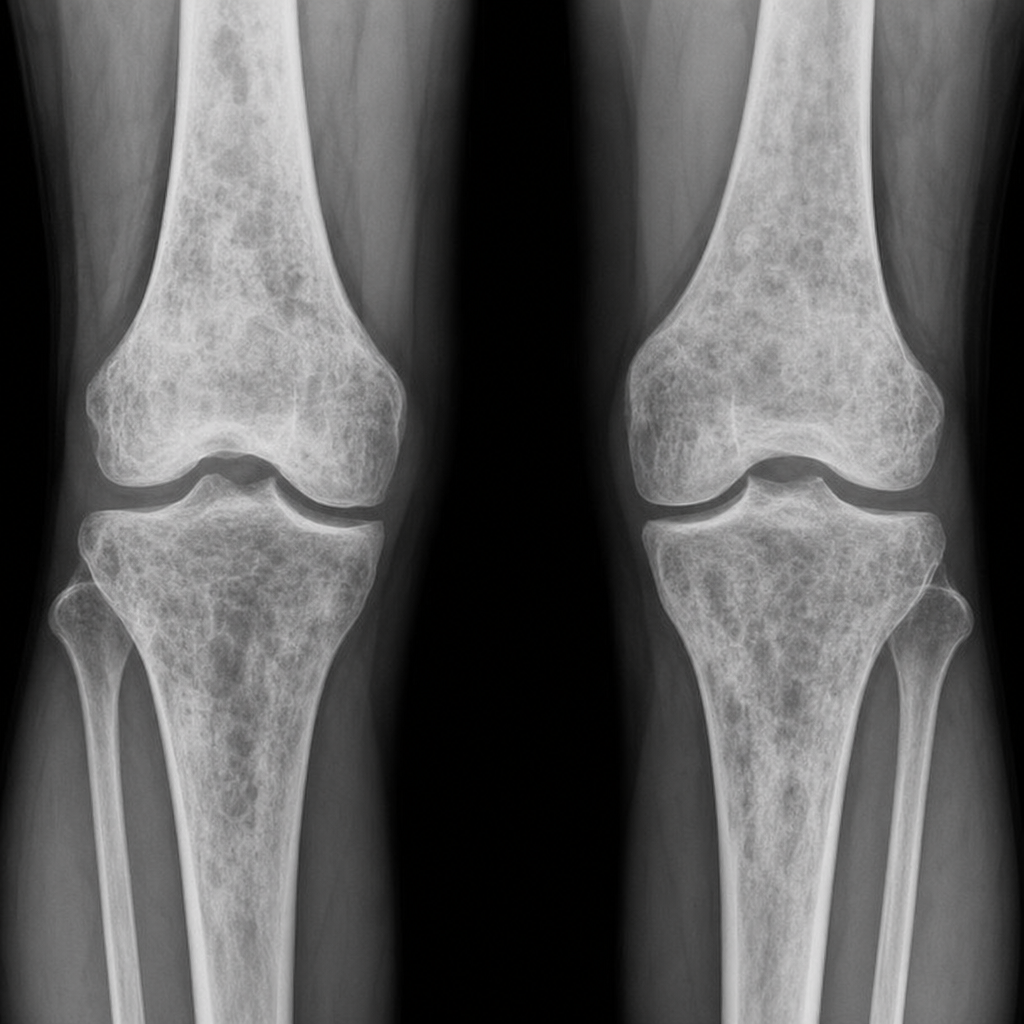
A 35-year-old man presented with knee pain. The x-ray of his knee joint is given below. What is the probable diagnosis?
A patient with systemic mastocytosis undergoes skeletal survey. Which radiological finding is most characteristic of skeletal involvement?
An MRI pelvis shows 'bow tie' sign in the sacrum. Which additional finding would best support sacral insufficiency fracture?
Practice by Chapter
Radiographic Anatomy of Bones and Joints
Practice Questions
Imaging of Fractures and Dislocations
Practice Questions
Arthritides: Inflammatory and Degenerative
Practice Questions
Metabolic Bone Diseases
Practice Questions
Bone and Soft Tissue Tumors
Practice Questions
Congenital Skeletal Anomalies
Practice Questions
Spine Imaging
Practice Questions
Skeletal Infections
Practice Questions
Sports Medicine Imaging
Practice Questions
Imaging of Prostheses and Implants
Practice Questions
Musculoskeletal Ultrasound
Practice Questions
MSK Interventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app