
Musculoskeletal Radiology — MCQs

On this page
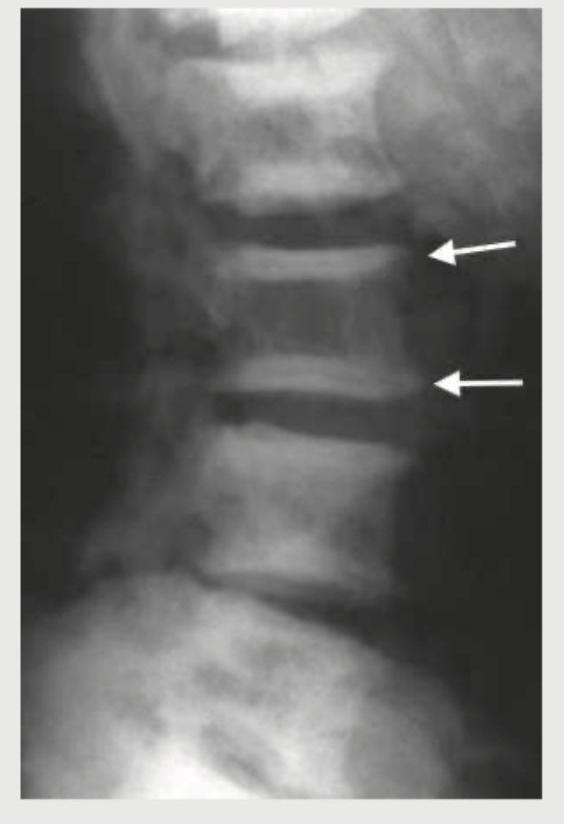
The image of X-ray spine shows?

Identify the defect shown in the X-ray skull:
The X-ray of the patient shows?

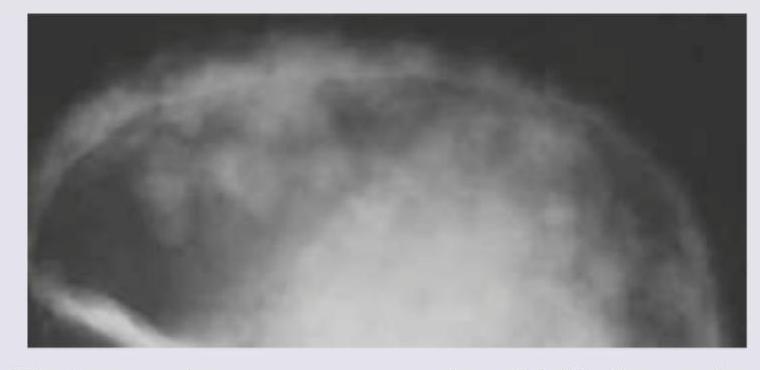
The following Skull X-ray is seen in:
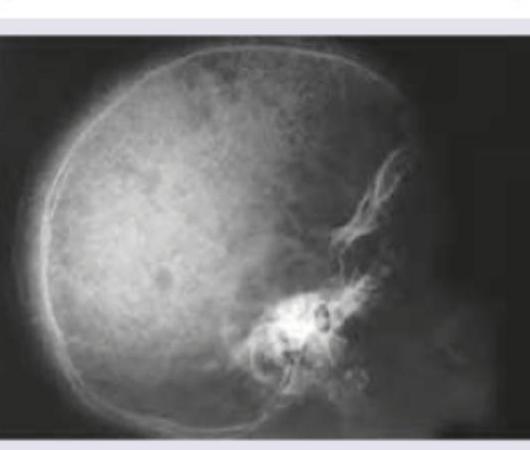
A child presents with severe microcytic anemia, hepatosplenomegaly, and elevated HbF on hemoglobin electrophoresis. The following X-ray skull shows:

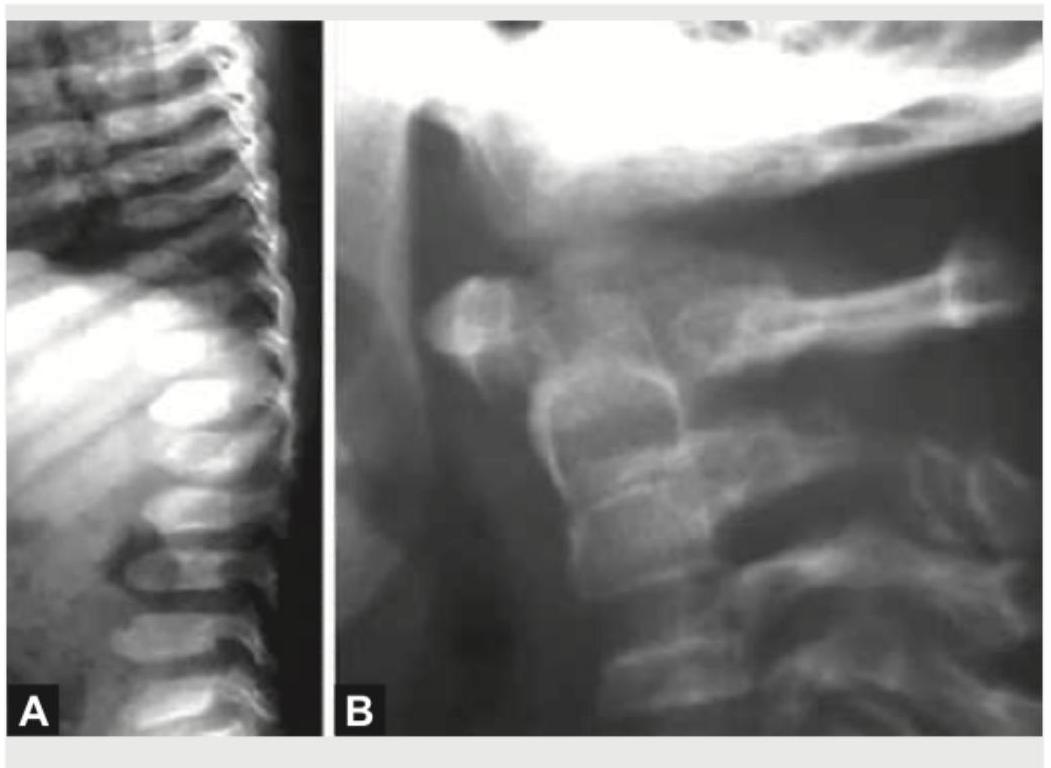
Comment on the diagnosis based on X-ray spine findings:
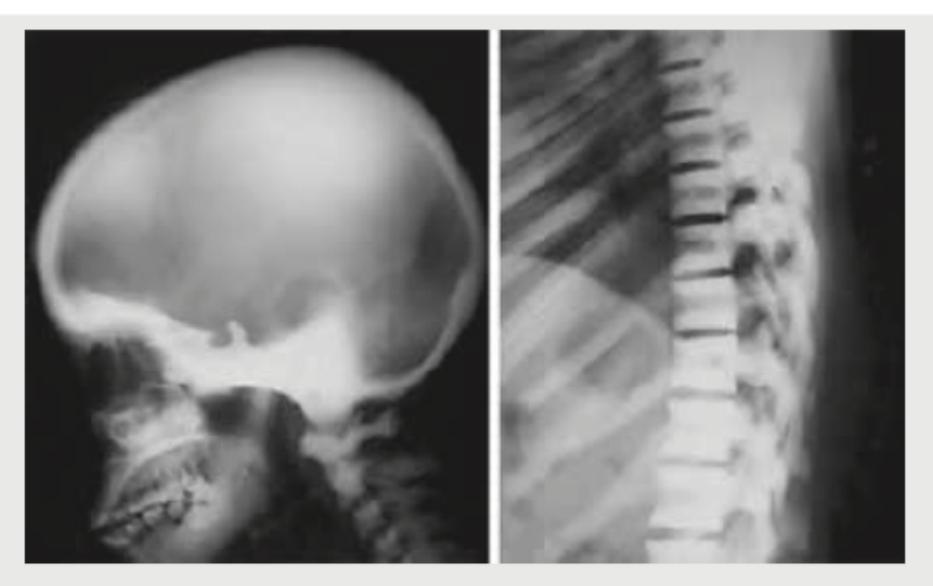
Comment on the diagnosis based on the skull and vertebral changes shown in the radiological image below:
A 28-year-old female with chronic kidney disease presents with bone pain and elevated parathyroid hormone levels. She has a history of renal stones. What is the sign visible in the image?
What does the following radiograph show?

The X-ray and MRI findings given below point to the diagnosis of: (Recent NEET Pattern 2016-17)

Practice by Chapter
Radiographic Anatomy of Bones and Joints
Practice Questions
Imaging of Fractures and Dislocations
Practice Questions
Arthritides: Inflammatory and Degenerative
Practice Questions
Metabolic Bone Diseases
Practice Questions
Bone and Soft Tissue Tumors
Practice Questions
Congenital Skeletal Anomalies
Practice Questions
Spine Imaging
Practice Questions
Skeletal Infections
Practice Questions
Sports Medicine Imaging
Practice Questions
Imaging of Prostheses and Implants
Practice Questions
Musculoskeletal Ultrasound
Practice Questions
MSK Interventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app