
Musculoskeletal Radiology — MCQs

On this page
Honda or H sign on STIR MRI is characteristic of which condition?
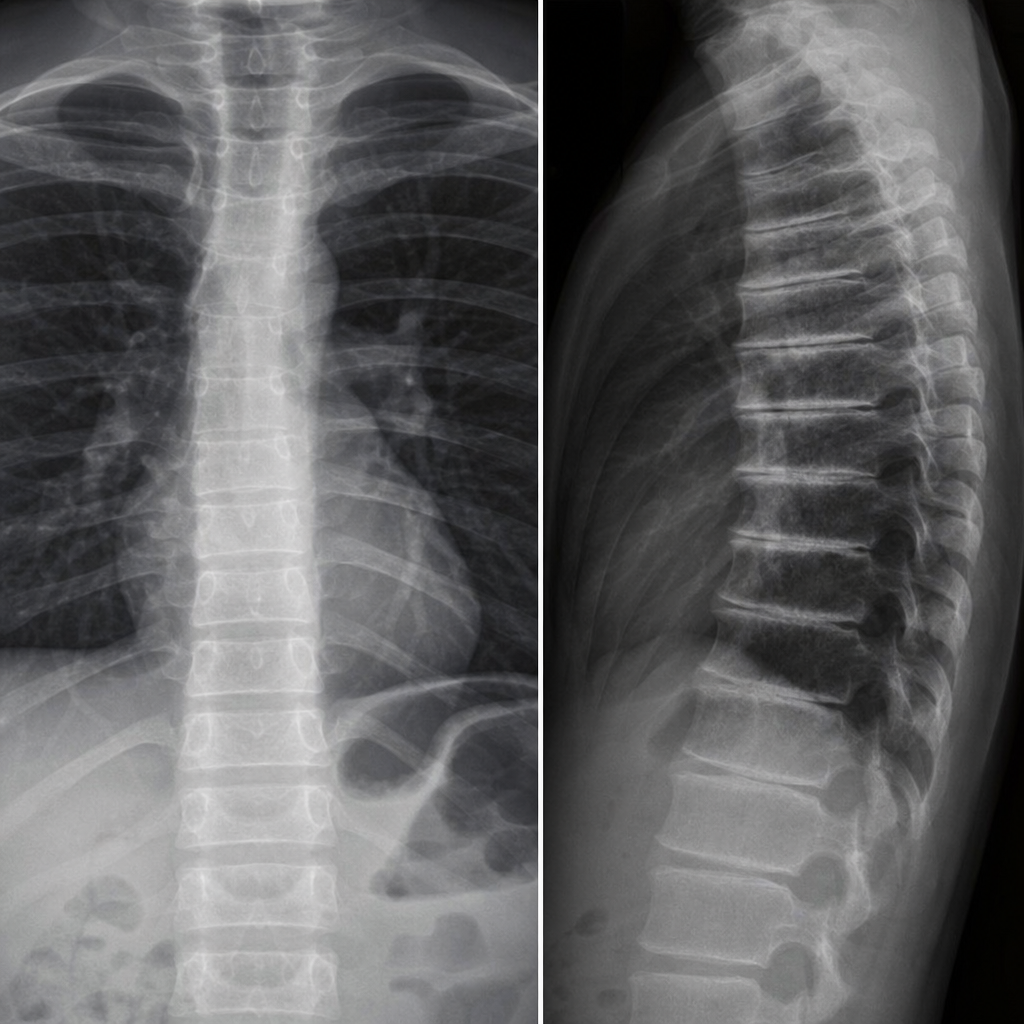
A 56-year-old female presents with chronic lower back pain. A lateral lumbar spine X-ray is provided. Based on the radiological findings, which of the following is the most likely diagnosis?
Which is the earliest imaging modality used to detect ankylosing spondylitis?
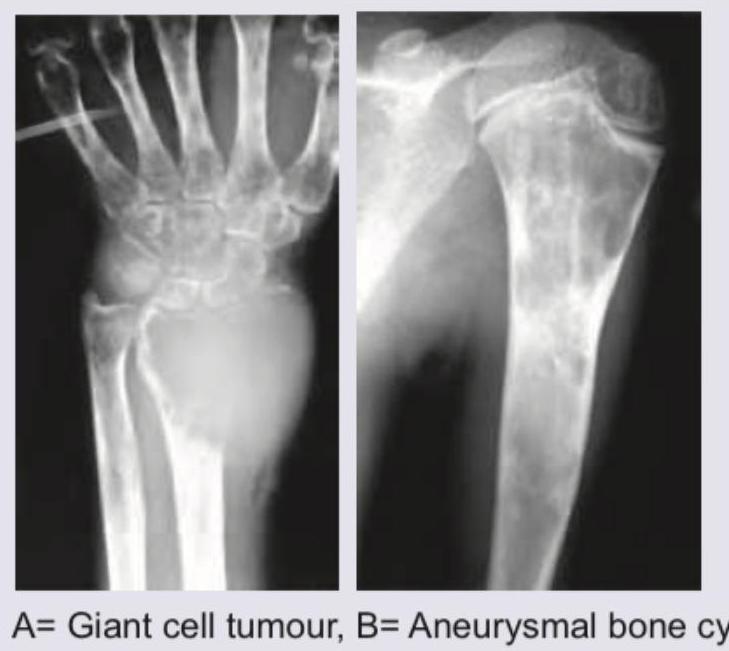
What are the correct diagnoses for lesions A and B shown in the image?
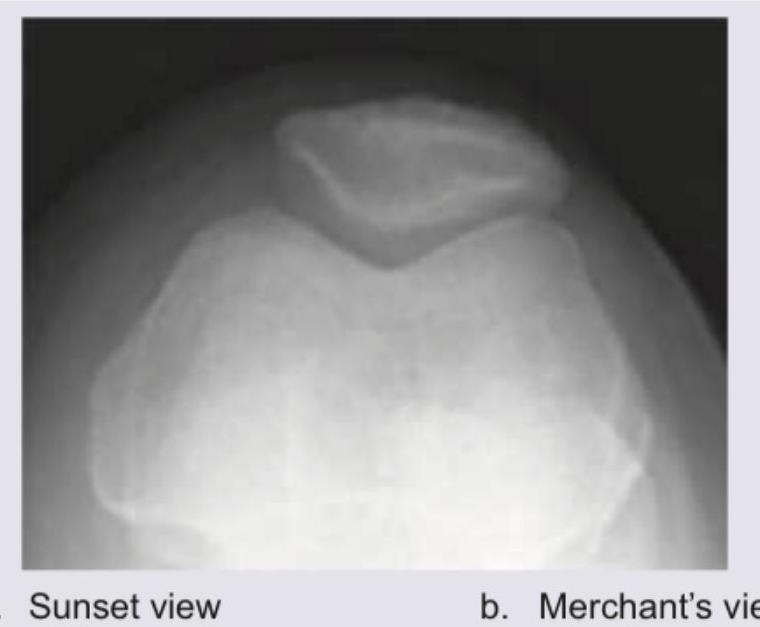
The following view of the knee joint is known as: (The image was obtained with the patient supine, knee flexed at approximately 30–60°, and the X-ray beam directed tangentially along the long axis of the patella from the foot end upward.)
What is correct about the finding in X-ray shoulder?

What is the correct diagnosis for the image shown?
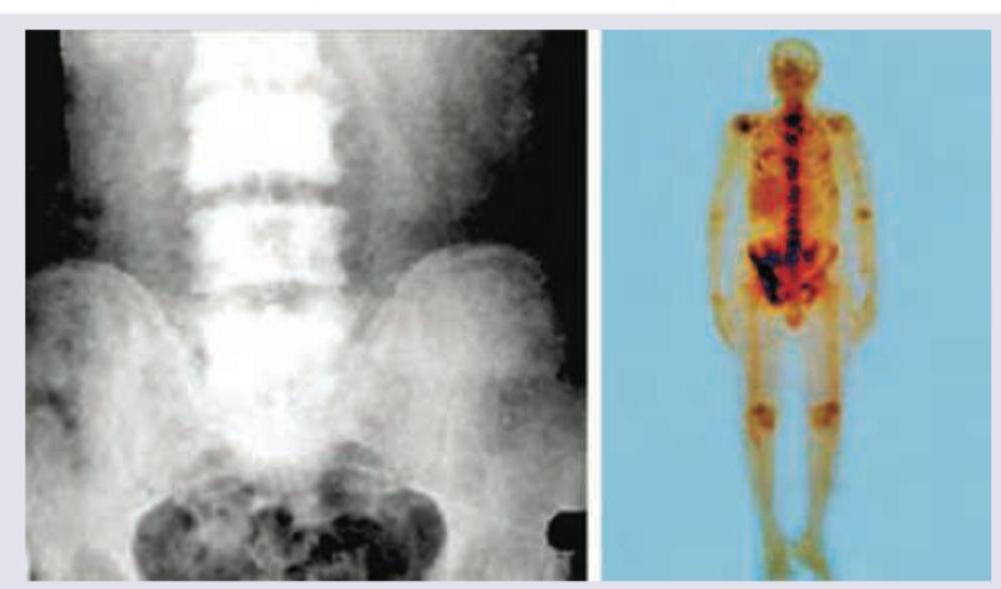
Which of the following best describes the image shown in patient with carcinoma prostate?
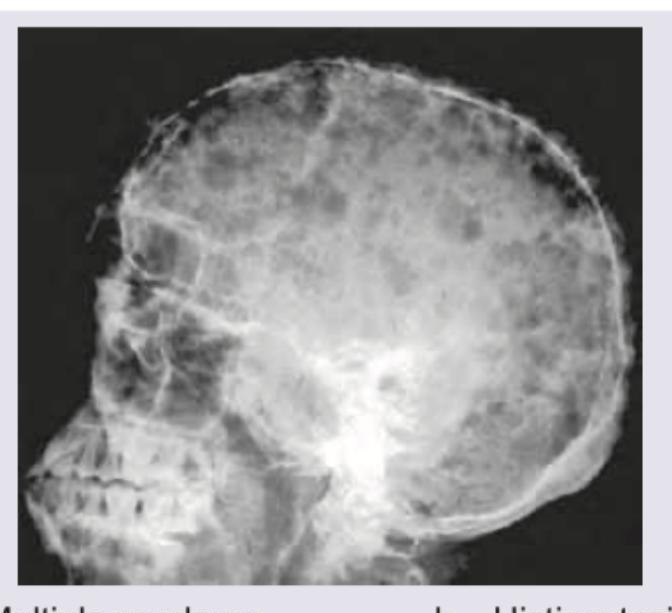
The findings in the following skull X-ray are most characteristic of:
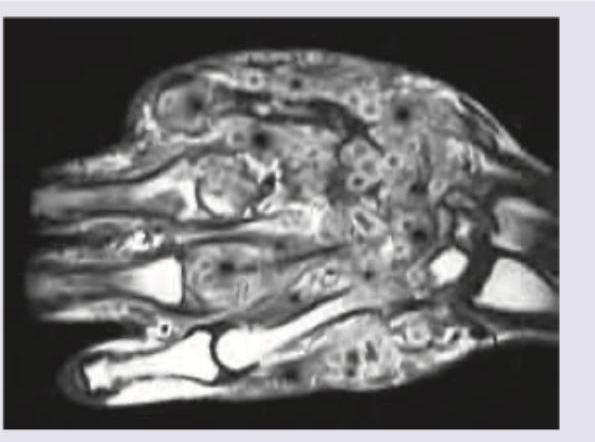
What is the most likely diagnosis based on the MRI findings?
Practice by Chapter
Radiographic Anatomy of Bones and Joints
Practice Questions
Imaging of Fractures and Dislocations
Practice Questions
Arthritides: Inflammatory and Degenerative
Practice Questions
Metabolic Bone Diseases
Practice Questions
Bone and Soft Tissue Tumors
Practice Questions
Congenital Skeletal Anomalies
Practice Questions
Spine Imaging
Practice Questions
Skeletal Infections
Practice Questions
Sports Medicine Imaging
Practice Questions
Imaging of Prostheses and Implants
Practice Questions
Musculoskeletal Ultrasound
Practice Questions
MSK Interventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app