
Musculoskeletal Radiology — MCQs

On this page
Trolly tract sign is seen in which of the following conditions?
What is the best method to evaluate a discrepancy in the articular disc of the temporomandibular joint (TMJ)?
A 76-year-old man presents with a lytic lesion in the vertebrae. X-ray of the skull showed multiple punched-out lesions. What is the most likely diagnosis?
An oblique view in an X-ray of the hand is required for the diagnosis of which carpal bone?
What is seen in the X-ray of the femur below?

What is seen in the X-ray of the femur below?

What is seen in the X-ray of the femur below?

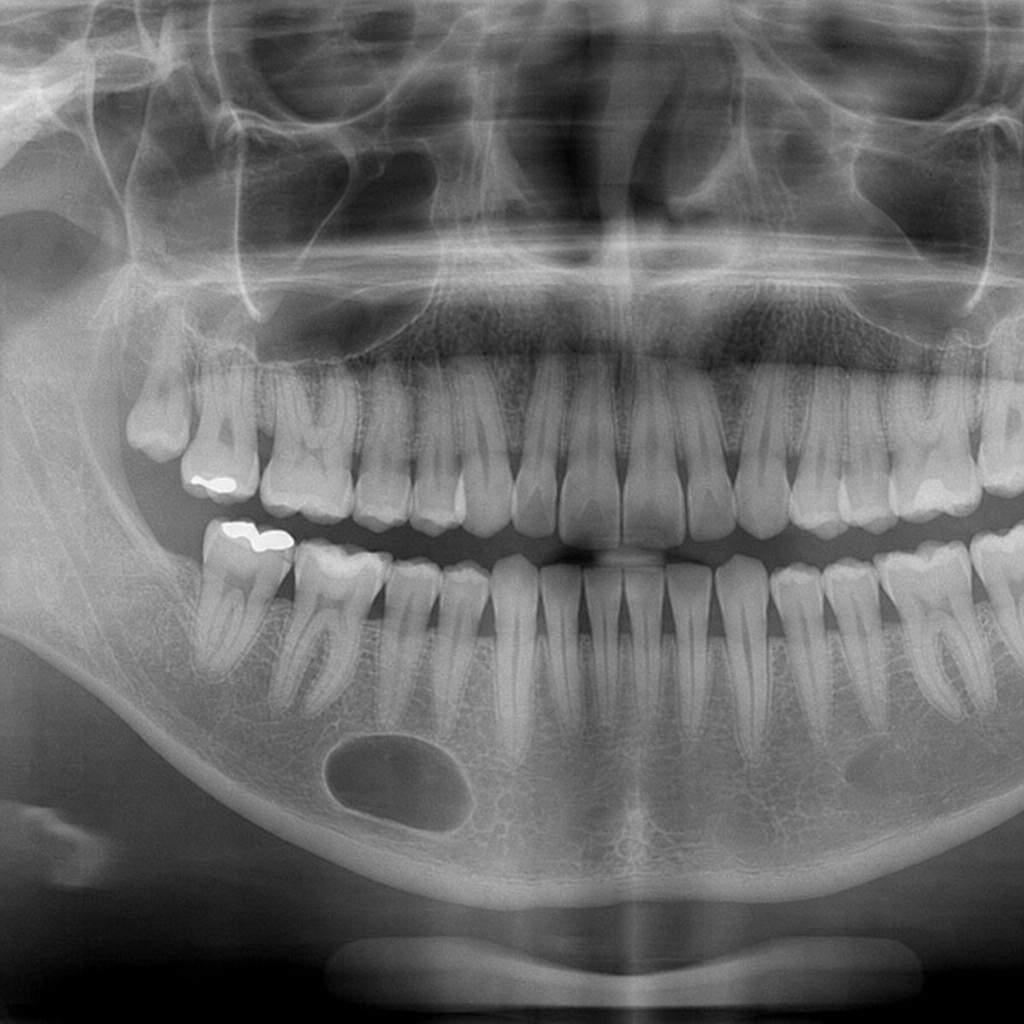
A radiograph of a 32-year-old patient reveals an asymptomatic lesion that was an accidental finding. What is the most likely diagnosis?
Based on the provided MRI image of the knee (A), which shows a well-defined fluid collection below the patella and superficial to the patellar tendon, what is the most likely diagnosis?
Based on the provided X-ray image, identify the most likely diagnosis.
Practice by Chapter
Radiographic Anatomy of Bones and Joints
Practice Questions
Imaging of Fractures and Dislocations
Practice Questions
Arthritides: Inflammatory and Degenerative
Practice Questions
Metabolic Bone Diseases
Practice Questions
Bone and Soft Tissue Tumors
Practice Questions
Congenital Skeletal Anomalies
Practice Questions
Spine Imaging
Practice Questions
Skeletal Infections
Practice Questions
Sports Medicine Imaging
Practice Questions
Imaging of Prostheses and Implants
Practice Questions
Musculoskeletal Ultrasound
Practice Questions
MSK Interventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app