
Musculoskeletal Radiology — MCQs

On this page
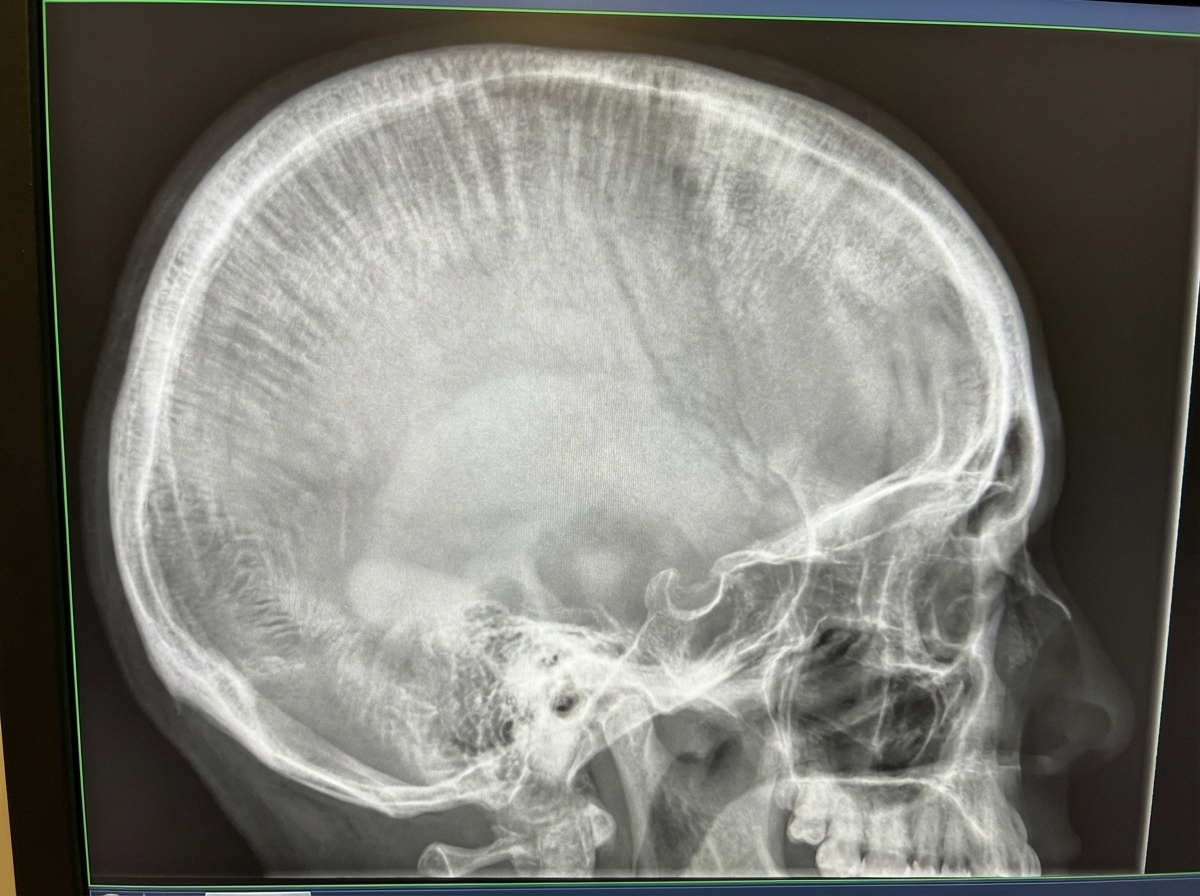
Wide diploic space of the skull with a brush border (hair on end) appearance is characteristic of which condition?
Which of the following conditions can manifest with the shown X-ray findings in the skull?
Osteoblastic metastases commonly arise from which primary tumor?
What is the characteristic radiological finding of Ewing's sarcoma?
Intraosseous skeletal tumors are best diagnosed by which imaging modality?
Maclean's sign is seen in which of the following conditions?
Multiple periapical radiolucencies are seen in which of the following conditions?
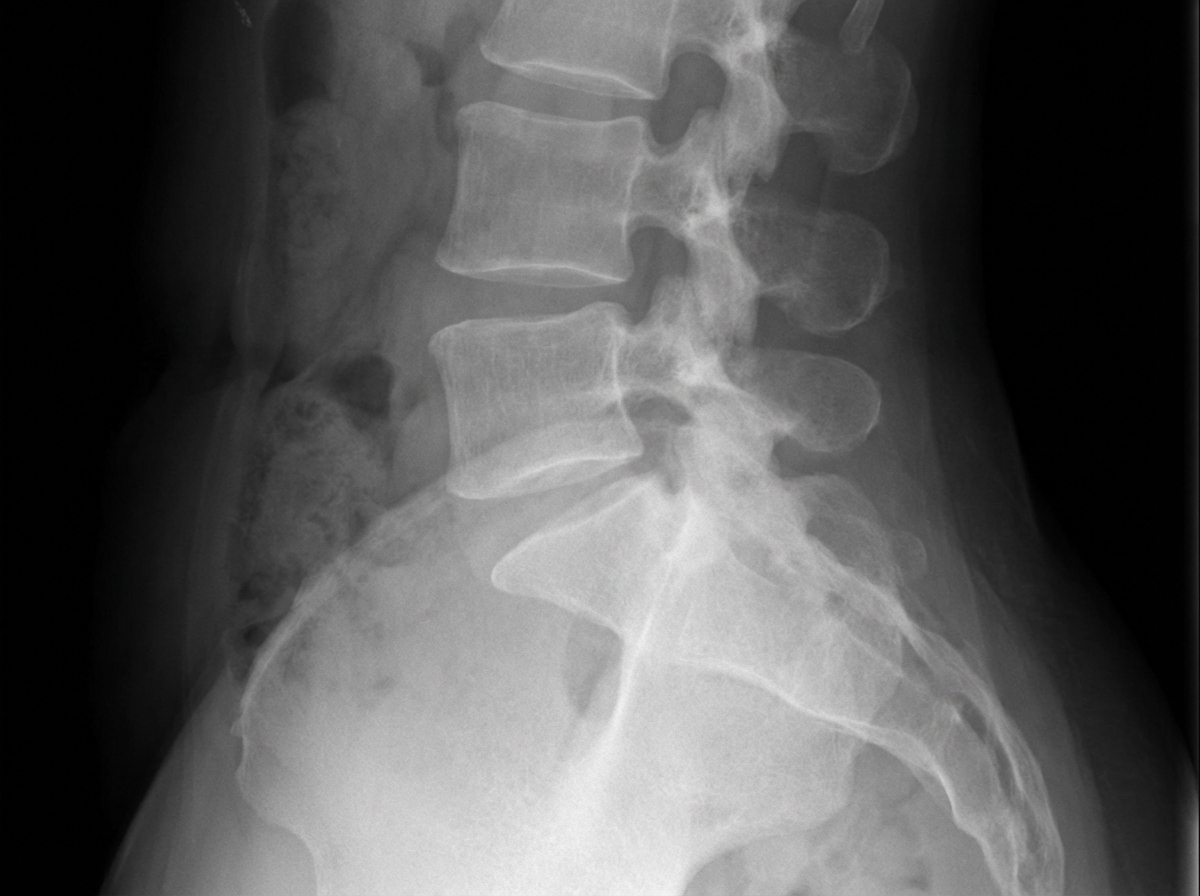
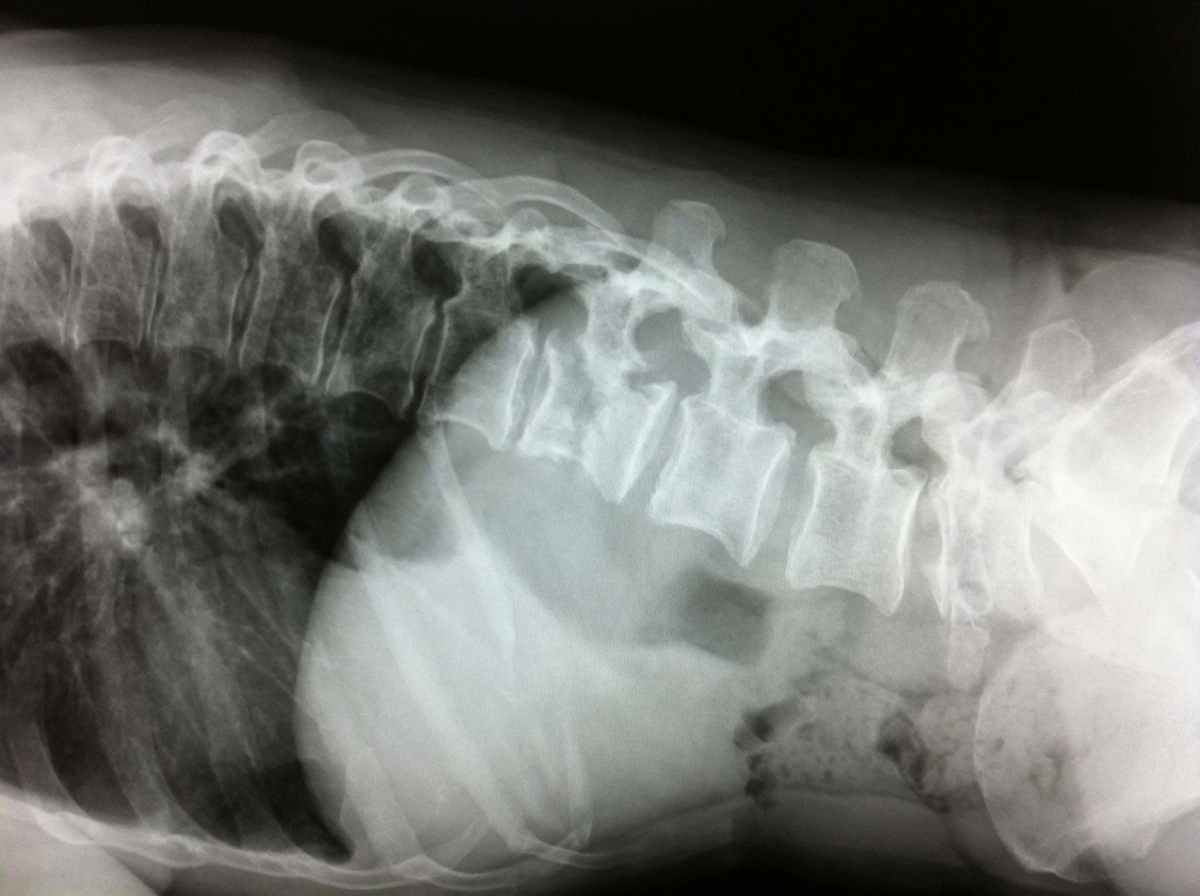
A lateral view X-ray of the lumbosacral spine shows which of the following findings?
A Judet view on an X-ray is primarily used for visualizing injuries to which anatomical structure?
A 35-year-old male from a TB-endemic region presents with a 3-month history of back pain, low-grade fever, night sweats, and weight loss. ESR is elevated at 85 mm/hr and Mantoux test is strongly positive. Which of the following is the most probable diagnosis?
Practice by Chapter
Radiographic Anatomy of Bones and Joints
Practice Questions
Imaging of Fractures and Dislocations
Practice Questions
Arthritides: Inflammatory and Degenerative
Practice Questions
Metabolic Bone Diseases
Practice Questions
Bone and Soft Tissue Tumors
Practice Questions
Congenital Skeletal Anomalies
Practice Questions
Spine Imaging
Practice Questions
Skeletal Infections
Practice Questions
Sports Medicine Imaging
Practice Questions
Imaging of Prostheses and Implants
Practice Questions
Musculoskeletal Ultrasound
Practice Questions
MSK Interventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app